Study highlights need for improved screening in anorectal malformation patients
A recent study from the Division of Colorectal and Pelvic Reconstruction at Children’s National Hospital, led by Chief Marc Levitt, MD, explores the prevalence of additional abnormalities in children born with anorectal malformations (ARM). While many of these abnormalities co-occur, including vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula or esophageal atresia, renal defects and limb defects, known as the VACTERL association, the study reveals that some critical anomalies, particularly spinal cord and gynecologic malformations, are often missed, an oversight that can significantly affect patient outcomes.
What it means
This multi-institutional retrospective study aimed to assess the effectiveness of current diagnostic criteria for VACTERL screening in ARM patients and to identify anomalies that are at risk of being overlooked. The researchers utilized data from the Pediatric Health Information Systems database, which includes over 100 children’s hospitals, to analyze a wide range of associated abnormalities in ARM across the United States.
The findings highlight that the most common anomalies in ARM patients include cardiac, vertebral/spinal, renal and gynecologic (in females). While many of these anomalies are diagnosed at birth, the study suggests that some are identified only later in a patient’s care, pointing to a gap in early screening, particularly for spinal cord and gynecologic issues.
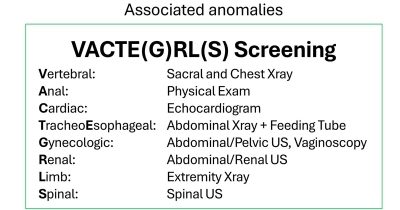
Based on the study’s results, the authors propose an expansion of the VACTERL acronym to VACTE(G)RLS to stress the importance of gynecologic (G) and spinal cord anomalies (S) in ARM patients.
Based on the study’s results, the authors propose an expansion of the VACTERL acronym to VACTE(G)RLS to stress the importance of gynecologic (G) and spinal cord anomalies (S) in ARM patients. This expanded acronym would help ensure that both surgical and non-surgical providers are aware of these often-missed malformations, improving early diagnosis and intervention.
Why it matters
Although other studies have examined the prevalence of VACTERL anomalies in ARM patients, this is the first to compare diagnosis rates at birth with diagnoses made later during subsequent hospital admissions. Timely identification of these associated malformations is crucial for early intervention in females, as untreated gynecologic anomalies can lead to reproductive issues later in life and for patients with spinal conditions that require intervention.
The proposed change to the standard usage VACTERL acronym underscores the significance and frequency of these malformations happening in combination, potentially leading to improved screening protocols and, ultimately, better patient outcomes. By emphasizing the importance of comprehensive screening at birth, the study advocates for a more thorough approach to diagnosing ARM-associated anomalies, which can significantly enhance long-term care for these patients.
Authors from Children’s National include – Thomas Xu, MD, Andrea Badillo, MD, Briony Varda, MD, MPH, Christina Feng, MD, and Marc Levitt, MD.
You can read the full study, VACTERL screening in newborns with anorectal malformations – an opportunity to optimize screening practices, add gynecologic and spinal conditions, and utilize a new acronym: VACTE(G)RLS, in the Journal of Pediatric Surgery.