Despite research showing how vital advance care planning conversations are between adolescents with cancer and their families, the efficacy of pediatric advance care planning has not been studied in Hispanic adolescents living with cancer.
Pediatric advance care planning has positively impacted English-speaking adolescents with cancer and HIV, but it has not been studied in other populations — exacerbating health disparities. In a new study published in Clinical Practice in Pediatric Psychology, Maureen E. Lyon, Ph.D., lead author and clinical health psychologist at Children’s National Hospital, and other experts look to adapt and refine the evidence-based Family-Centered Advance Care Planning for Teens with Cancer (FACE®-TC) for Spanish-speaking adolescents with cancer. Using a community-based participatory approach and key informant interviews with patients and families, the experts identified important themes and outcomes.
Despite research showing how vital advance care planning conversations are between adolescents with cancer and their families, the efficacy of pediatric advance care planning has not been studied in Hispanic adolescents living with cancer. According to the authors, this creates a health disparity as Hispanic adolescents with cancer and their families do not have access to or provision of this potentially beneficial service.
“If successfully adapted, FACE-TC Spanish would benefit patient’s communication with their families about their end-of-life treatment preferences if the worse were to happen and they could not communicate,” Dr. Lyon said. “It could also increase families’ positive appraisal of their caregiving and increase communication about goals of care with treating physicians, so the first conversation about goals of care is not in the intensive care unit.”
The study’s findings showed that first-generation Spanish-speaking individuals living in the Washington D.C., Maryland and Virginia area wanted community education about advance care planning for Spanish-speaking adults, many of whom were unfamiliar with the concept.
These findings, in turn, showed the need for future research to include informational messages on Hispanic radio stations, educational workshops or radionovelas.
“We learned that fear of deportation meant that potential participants only felt safe to participate while at the hospital,” Dr. Lyon added. “Because of COVID-19, this was not feasible during the study period. There was consensus that families should be involved in the conversations and that the goals of care conversations and advance directives should be communicated to the physician.”
While this is the first study to adapt a family-centered approach to pediatric advance care planning for Spanish-speaking teens with cancer and their families, it is consistent with cultural values of ‘familismo’ (family) and ‘respecto’ (respect).
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/10/close-up-of-two-people-holding-hands.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-10-21 11:42:562021-10-21 11:42:56Effective palliative end-of-life care for Spanish-speaking teens with cancer
A study published in The Journal of Pediatrics finds an association between a teen’s preference for evening or morning activities, coupled with nightly sleep duration, influences how awake they feel behind the wheel.
Each year, around Daylight Saving Time, we set our clocks forward and reprogram our bodies to adjust to spring. While most people welcome warmer days and lingering daylight, the time transition – and losing an hour of sleep – may leave some feeling jet lag.
For teens, the time transition is even more pronounced. Due to an adolescent’s developing body and a release of hormones to support growth and development, their biological clock is naturally set for late-evening bedtimes. Getting enough sleep is tough, especially with packed activity schedules and early-morning school start times.
A new study in The Journal of Pediatrics finds the impact of student sleep deprivation extends past feeling alert in class. Almost half of teen drivers surveyed – 205 out of 431 – from Fairfax County Public Schools reported driving drowsy at least once during the 2015 school year, the study period. Out of the 431-person sample, 63.1 percent of respondents reported driving several times a week. One-third of participants drove every day.
Helping teens feel alert behind the wheel is two-fold: Healthy school start times, those starting at 8:30 a.m. or later, help. Getting enough sleep is critical. The researchers also found that a student’s chronotype, or their preference for morning or evening activities, based on the Morningness-Eveningness Scale for Children, factor into drowsy driving:
Students with an evening chronotype, or preference for evening activities, coupled with shorter school-night sleep duration, were more likely to experience sleep-impaired driving.
Students with a morning chronotype, and who got at least eight hours of sleep, had the lowest prevalence of drowsy driving.
Compared with students who slept for at least eight hours on school nights, those who slept for less than seven hours had a 13.9 percent higher prevalence of drowsy driving.
The mean age of students surveyed was 16.9 years. The mean range of school-night sleep was seven hours.
Daniel Lewin, Ph.D., associate director of sleep medicine at Children’s National Health System, encourages schools to adopt later school start times, which Fairfax County Public Schools did, and he encourages students and families to assess their sleep patterns – focusing not just on sleep quantity but on sleep quality. His advice for families or students hesitant to change is to start small.
Try a seven-day challenge: Sleep on a regular schedule, sleep for recommended amounts of time, based on age-appropriate guidelines, cut out naps and eliminate late-afternoon caffeine intake.
Most children and families will start to notice the immediate benefits of getting a good night’s sleep, especially throughout the week: less daytime sleepiness, happier moods, improved eating habits and feeling more alert behind the wheel, which impacts driver safety – and not just for teen drivers but for parents, teachers and everyone on the road.
Teens have a biological preference to fall asleep later than younger children and adults, and wake up later, due to a delayed release of hormones that promote sleep. This timing coincides with puberty and makes it harder for middle and high school students to fall asleep early – regardless of 5 a.m. alarms and 7:17 a.m. school start times.
After studying this trend among nearly 1,000 seventh and eighth-grade students in 11 middle schools within a Mid-Atlantic school district, Daniel Lewin, Ph.D., a sleep medicine specialist, pediatric psychologist and associate director of the sleep medicine program at Children’s National Health System, coauthored and published research entitled “Later Start, Longer Sleep: Implications of Middle School Start Times” in the Journal of School Health, which outlines the benefits of delaying school start times.
The research team divided students into two groups: Close to 650 students attended eight late-starting middle schools, where school started at 8 a.m., while nearly 350 students attended early-starting middle schools, where school started at 7:23 a.m.
Students starting school 37 minutes later, despite going to bed 15 minutes later than peers attending an earlier-starting school, got 17 minutes more sleep each night and were more likely to report feeling wide awake during class. The researchers predicted this later-starting school model would translate to students getting an extra 75 minutes of sleep a week – roughly 51 hours of extra sleep each school year. These researchers find that every two minutes in delayed school start times results in one minute of additional sleep each night for children and teens.
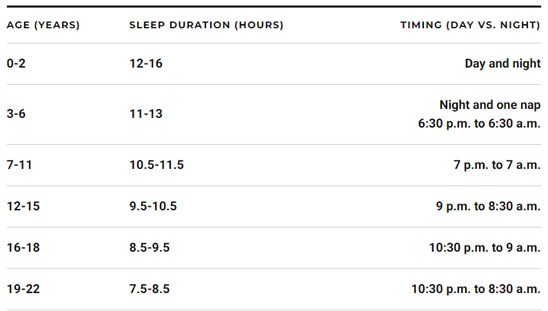
Middle and high school students should get 8.5 to 10.5 hours of sleep each night, ideally between 9 p.m. and 8:30 a.m. for 12- to 15-year-olds and 10:30 p.m. and 9 a.m. for 16- to 18-year-olds.
The American Academy of Pediatrics (AAP) published similar research in their journal, Pediatrics, about the benefits of letting teens catch up on sleep, citing a reduced risk of students being overweight, getting into car accidents or suffering from depression as well as a greater likelihood of having better grades, higher test scores and a better quality of life. AAP recommends schools start at 8:30 a.m. or later to allow students to get 8.5 to 9.5 hours of sleep each night and issued a statement in 2014, entitled “School Start Times for Adolescents.”
Dr. Lewin continues to track these benefits and works with schools to implement the changes. He recently wrote an editorial, entitled “All the Clocks Are Ticking: Sleep Health and Metabolism,” for the Journal of Adolescent Health about the correlation between improved sleep health, mental and physical health and academic performance, explaining how circadian clocks, present on a cellular level, influence behavior and metabolism.
While pushing school start times back requires an immediate investment of rearranging travel routes, bell schedules and after-school activities, several school districts near Washington, D.C., from Virginia Beach to Fairfax County, are adopting this public health model.
An economic analysis conducted by the RAND Corporation finds that after two years, the benefits of reorganizing school start times outweigh the costs.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/General-school-supplies.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-10 07:00:302021-10-25 11:56:40Studying the impact of later school start times
Ongoing research is helping to define the broad spectrum and multi-faceted nature of type 2 diabetes in terms of its presentation, its rapidity of progression and its underlying genetic susceptibilities. In a recent study of 8,980 adults published in The Lancet, diabetes was further classified into five clusters, ranging from insulin-deficient, typically referred to as type 1, to groups of patients with primary insulin-resistance, traditionally classified as type 2 diabetes, with the caveat that each cluster had a distinct risk profile for disease progression and risk for diabetes complications.
Moreover, investigators have recently demonstrated, through the Restoring Insulin Secretion (RISE) Consortium, that youth compared to adults with early type 2 diabetes have greater insulin resistance relative to insulin secretion. Understanding variances on the diabetes spectrum, especially as it relates to risk for disease progression in youth, helps researchers develop targeted therapies that may help reduce complications and the burden of this chronic disease.
Ongoing research
Stephanie Chung, M.B.B.S., a pediatric endocrinologist at the National Institutes of Health and an adjunct assistant professor of pediatrics at Children’s National, is one researcher who hopes to use this knowledge to transform public health outcomes. Dr. Chung is studying how teens and young adults with severe insulin-resistant diabetes (SIRD) respond to new treatment, paired with lifestyle-based interventions.
Here is a Q&A with Dr. Chung about her latest research:
Tell Innovation District readers more about your diabetes research. How has your previous research influenced this study?
My research and publications are focused on understanding how genes, environment and lifestyle factors contribute to the pathology of diabetes, obesity and insulin resistance in populations of African descent and on identifying more effective screening and treatment options.
We know that African-American youth with type 2 diabetes have the highest complication and treatment failure rates among minority youth. However, the reasons underlying this health disparity are still not fully understood. Metformin, the only approved oral diabetes treatment for youth with type 2 diabetes, works less than half of the time in African-American youth. Although new evidence suggests that gut bacteria and genetics may influence the efficacy of metformin, this data is insufficient in African-American youth.
What is your goal with this diabetes clinical study?
The primary objective of this new study, entitled Therapeutic Targets in African-American Youth with Type 2 Diabetes, is to compare the combination of metformin and liraglutide versus metformin alone to reduce excess glucose produced by the liver in African-American youth with type 2 diabetes.
Additional objectives will evaluate the mechanism of action in the liver of these two agents and the influence of genetics and gut bacteria. This project brings together the research expertise of the National Institute of Diabetes and Digestive and Kidney Diseases, the National Human Genome Research Institute and the Children’s National.
Do you envision this type of dual therapy, a combination of drugs and lifestyle interventions, will serve as a bridge to optimal insulin function?
While metformin, diet and lifestyle changes remain the mainstay of diabetes treatment, our study will evaluate whether this combination regimen could help to slow the progression of type 2 diabetes in African American youth. Our ultimate goal is the development of new precision medicine treatment options that can address the disparities in outcomes for African-American youth with type 2 diabetes.
What lessons do you see participants learning as they progress through the trial?
Our patients and their families are equal partners in care. Our comprehensive team of doctors, nurses, dietitians and counselors work closely with the patients and their families to help empower them to take charge of managing their diabetes. We teach them skills that include regularly monitoring their blood glucose levels and understanding how their activity and foods affect these levels. They are coached on making healthy food choices and incorporating exercise into their daily lives.
How do you teach children and teens about how their body responds to different foods?
This education starts as soon as participants enter the study. While patients are at the NIH for the inpatient study, we provide them with meals containing different ratios of carbohydrates, proteins, and fats and help them to analyze how their blood sugar responds to these levels, both before and after they take the medication. This type of education is important since participants will also have to monitor their blood sugar twice a day at home during the study. Most of the time, we use real-life situations as teaching moments. For example, if a participant had pizza for dinner, we will discuss with them why their blood sugar spiked and suggest alternative food choices. We provide this type of coaching every week. I often joke that after three months they become tired of hearing from us. But one of the strengths of this study is that participants receive personalized feedback that enables them to make healthy food choices for the rest of their life.
Can you tell us more about targeted food choices for teens?
A very enlightening procedure that we conduct on all of our study participants is measuring their basal metabolic rate (energy expenditure at rest). We show them how many calories they need to consume each day to maintain their body’s normal functions and compare that number with an estimate of how many calories they usually consume in a day. For many participants this is the first time that they have insight into the reasons for their weight gain.
How does this lab work help with meal planning?
After we create a participant’s metabolic chart we make food plans that support their lifestyle and caloric needs and are realistic to follow. For example, a 2,000 calorie per day diet can be separated into 400 calories for breakfast, 600 calories for lunch, 200 calories for snack and 800 calories for dinner.
How do you envision personalizing the field of diabetes research and treatment?
A precision medicine approach to type 2 diabetes will help us to better explore if and how factors like genes, environment and lifestyle impact insulin and glucose metabolism in populations with significant treatment outcomes disparities. With this approach we hope to uncover novel targeted treatment and prevention strategies that demonstrate more efficacy and cost-efficiency than current treatment approaches for high-risk populations.
Where can people learn more about the trial?
Learn more about the study by watching this informational video. If you’re interested in joining the study, please contact the NIH Office of Clinical Trial Recruitment at 866-999-1116.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/10/boy-on-a-treadmill.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-10-04 12:17:152020-05-04 10:08:54Therapeutic targets in African-American youth with type 2 diabetes