
Marshall Summar, M.D., receives Lifetime Achievement Award for rare disease work

For making strides to improve the lives of the rare disease community, the National Organization for Rare Disorders (NORD®) recognized Marshall Summar, M.D., with a Lifetime Achievement Award.
For making strides to improve the lives of the rare disease community, the National Organization for Rare Disorders (NORD®) recognized Marshall Summar, M.D., chief of the Division of Genetics and Metabolism and the director of the Rare Disease Institute at Children’s National Hospital, with a Lifetime Achievement Award.
This award honors individuals for outstanding career-long achievement on behalf of the rare disease community and commitment to improving the lives of those affected by rare diseases. It has been presented only a few times over NORD’s nearly 40-year history, most recently to former NIH Director Francis Collins, M.D., Ph.D., in 2015 and to clinician and researcher Robert Campbell, M.D., of Children’s Hospital of Philadelphia in 2018.
“I am honored to receive this award from NORD. It is so special to be recognized by the leading rare disease organization. This award comes from the work of so many people over the years, particularly our great team at Children’s National,” said Dr. Summar. “This acknowledgement of what we have done to date just gets me more excited about the future!”
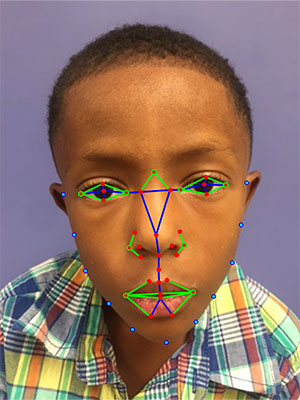
Dr. Summar developed and launched the world’s first Rare Disease Institute at Children’s National in 2017, which is now located on the Children’s National Research & Innovation Campus, a first-of-its-kind pediatric research and innovation hub in Washington, D.C.
The institute, which includes the largest clinical group of pediatric geneticists in the nation, focuses on developing the clinical care field of the more than 8,000 rare diseases currently recognized and advancing the best possible treatments for children with these diseases.

Marshall and Karen Summar.
“Dr. Summar’s passion for serving patients is at the core of everything he does,” said Debra Regier, M.D., medical director of the Rare Disease Institute. “His mentorship for the next generation of medical and biochemical geneticists has become his legacy.”
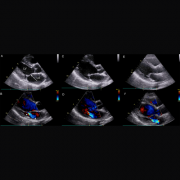
The work Dr. Summar has done over the course of his career has resulted in new drugs in FDA trials for patients with congenital heart disease and premature birth. He also holds more than 60 patents and has published more than 160 peer-reviewed research studies.
“Beginning with his work as a clinician in the 1980s, Dr. Marshall Summar has spent a career forging partnerships, advocating at the highest level and developing new ways to treat rare disease patients,” said Peter L. Saltonstall, president and CEO of NORD.
“Dr. Summar served on the NORD Board of Directors for nine years, including six years as Chairman, and so we at NORD have been lucky enough to have years of firsthand experience with his leadership, community-building and innovation efforts in the rare disease field. This award is a recognition and appreciation for sustained excellence, including critical work with organizations such as the American College of Medical Genetics, the National Institutes of Health, NORD, and the Rare Disease Institute at Children’s National. For decades of commitment to families and organizations combating rare diseases, NORD is thrilled to present the Lifetime Achievement Award to Dr. Marshall Summar at the 2022 Rare Impact Awards,” Saltonstall added.
Learn more about the Rare Disease Institute at Children’s National.























 Marshall Summar, MD
Marshall Summar, MD