Born to young parents, no prenatal testing had suggested any problems with Bella’s brain. But just a few hours after birth, Bella suffered her first seizure – one of many that would follow in the ensuing days. After brain imaging, her doctors in Iowa diagnosed her with hemimegalencephaly.
Strokes are neurologically devastating events, cutting off life-sustaining oxygen to regions of the brain. If these brain tissues are deprived of oxygen long enough, they die, leading to critical loss of function – and sometimes loss of life.
“As physicians, we’re taught to prevent or treat stroke. We’re never taught to inflict it,” says Taeun Chang, M.D., director of the Neonatal Neurology and Neonatal Neurocritical Care Program at Children’s National Hospital.
That’s why a treatment developed at Children’s National for a rare brain condition called hemimegalencephaly is so surprising, Dr. Chang explains. By inflicting controlled, targeted strokes, Children’s National physician-researchers have treated five newborns born with intractable seizures due to hemimegalencephaly before they’re eligible for epilepsy surgery, the standard of care. In the four surviving infants, the procedures drastically reduced or completely relieved the infants of hemimegalencephaly’s characteristic, uncontrollable seizures.
The most recent patient to receive this life-changing procedure is Bella, a 13-month-old from Iowa whose treatment at Children’s National began within her second week of life. Born to young parents, no prenatal testing had suggested any problems with Bella’s brain. But just a few hours after birth, Bella suffered her first seizure – one of many that would follow in the ensuing days. After brain imaging, her doctors in Iowa diagnosed her with hemimegalencephaly.
A congenital condition occurring in just a handful of children born worldwide each year, hemimegalencephaly is marked by one brain hemisphere growing strikingly larger and dysplastic than the other, Dr. Chang explains. This abnormal half of the brain is highly vascularized, rippled with blood vessels needed to support the seizing brain. The most conspicuous symptoms of hemimegalencephaly are the numerous seizures that it causes, sometimes several in the course of an hour, which also may prevent the normal half of the brain from developing and learning.
Prior studies suggest early surgery achieves better developmental outcomes with one study reporting as much as a drop of 10-20 IQ points with every month delay in epilepsy surgery.
The standard treatment for unilateral megalencephaly is a dramatic procedure called a hemispherectomy, in which surgeons remove and disconnect the affected half of the brain, allowing the remaining half to take over its neurological duties. However, Dr. Chang says, implementing this procedure in infants younger than 3 months of age is highly dangerous. Excessive, potentially fatal blood loss is likely in infants younger than 3 months who have a highly vascularized brain in the setting of an immature coagulation system. That leaves their doctors with no choice but to wait until these infants are at least 3 months old, when they are more likely to survive the surgery.
However, five years ago, Dr. Chang and her colleagues came up with a different idea when a newborn continued to have several seizures per hour despite multiple IV seizure medications: Because strokes cause irreversible tissue death, it might be possible to effectively incapacitate the enlarged hemisphere from within by inflicting a stroke on purpose. At the very least, this “functional embolization” might buy time for a traditional hemispherectomy, and slow or halt ongoing brain damage until the infants are able to withstand surgery. Ideally, this procedure may be all some children need, knocking out the offending hemisphere completely so they’d never need a hemispherectomy, which has late complications, such as hydrocephalus.
A pediatrician friend of Bella’s paternal grandparents read a story on Children’s National website about Darcy, another baby who’d received functional embolization a year earlier and was doing well. She contacted Dr. Chang to see if the procedure would be appropriate for Bella.
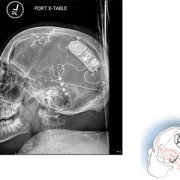
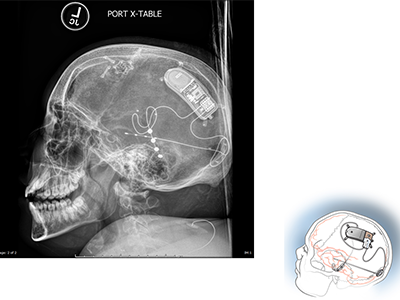
Within days, Bella and her family headed to Washington, D.C., to prepare for functional embolization herself. Within the first weeks of life, Bella underwent three separate procedures, each three to four hours long. Under real-time fluoroscopic and angiographic guidance, interventional neuroradiologist Monica Pearl, M.D., threaded a micro-catheter up from the baby’s femoral artery through the complex network of blood vessels all the way to her brain. There, in targeted branches of her cerebral arteries, Dr. Pearl strategically placed liquid embolic agent to obstruct blood flow to the abnormal half of Bella’s brain.
Immediately after the first procedure, the team had to contend with the same consequences that come after any stroke: brain swelling that can cause bleeding and herniation, complicated further by the already enlarged hemisphere of Bella’s brain. Using neuroprotective strategies learned from treating hundreds of brain-injured newborns, the neonatal neurocritical care team and the neonatal intensive care unit (NICU) minimized the brain swelling and protected the normal half of the brain by tightly controlling the brain temperature, her sugar and electrolyte levels, her blood pressure and coagulation system.
As the brain tissue in the oversized hemisphere died, so did the seizures that had plagued Bella since birth. She has not had a seizure since she left Children’s National more than one year ago. Her adoptive parents report that Bella is hitting many of the typical developmental milestones for her age: She’s getting ready to walk, blowing kisses and saying a few words. Physical, speech and occupational therapy will keep her moving in the right direction, Dr. Chang says.
“We believe that Children’s National is the only place in the world that’s treating newborns in this way to preserve their futures,” Dr. Chang says. “We’re privileged to be able to care for Bella and other kids with this rare condition.”
Bella’s transfer and successful procedures required the support and collective efforts of many within the hospital organization including William D. Gaillard, M.D., and his surgical epilepsy team; interventional neuroradiology with Dr. Monica Pearl; Neurosurgery; Neonatology and the NICU; social work; and even approval from Robin Steinhorn, M.D., senior vice president of the Center for Hospital-Based Specialties, and David Wessel, M.D., executive vice president and Chief Medical Officer.
“While obvious credit goes to the medical team who saved Bella’s future and the neonatal intensive care nurses who provided exceptional, intensive, one-on-one care, Bella’s team of supporters extend to all levels within our hospital,” Dr. Chang adds.
Also read:





 Several experts from Children’s National Hospital will be sharing their knowledge at the upcoming
Several experts from Children’s National Hospital will be sharing their knowledge at the upcoming 
 The choice between stereoelectroencephalography (SEEG) and subdural evaluation is not mutually exclusive, according to a new
The choice between stereoelectroencephalography (SEEG) and subdural evaluation is not mutually exclusive, according to a new