Predictive analytics elevates NICU patient care
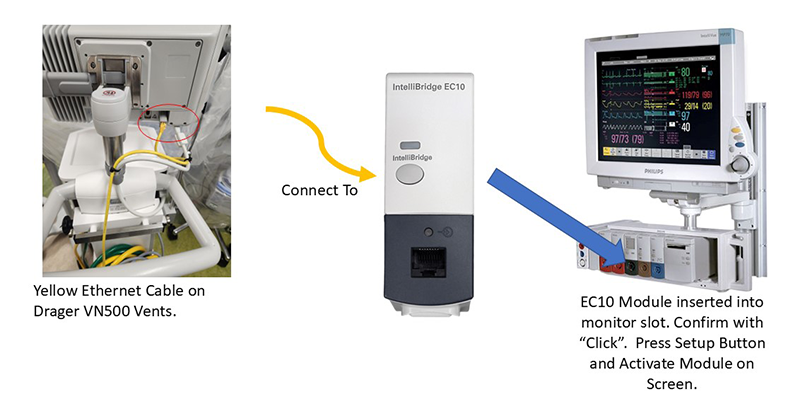
Connecting the Ventilator to Etiometry through the data acquisition module. ECS shown in red circle.
Managing the delicate health of premature infants in the NICU requires more than just vigilant care — it demands real-time insights and precision. With high-tech tools like the Etiometry platform, clinicians at Children’s National can now track changes in oxygen levels and other vital data, making timely adjustments to optimize each patient’s care.
Why it matters
This predictive analytics system allows doctors and nurses to visualize trends over time and collaborate seamlessly, even from a distance.
“By analyzing data and developing new algorithms, we can quickly identify if a patient is deteriorating, allowing us to intervene before further decline occurs. We can also fine-tune care, weaning patients who are ready faster and delaying it for those who aren’t, ultimately ensuring more targeted and effective treatment,” Lamia Soghier, MD, MED, MBA, neonatologist and the NICU Quality and Safety Officer.
How it works
“The technology relies on software and a piece of equipment called EC10, which connects ventilators to monitors. However, there aren’t enough of these devices to have one in each NICU room, leading to risks of misplacement or damage when patients move between rooms,” said Sofia Perazzo, MD, program lead for Neonatology at Children’s National.
“The $35,000 grant Children’s National received from the Founders Auxiliary Board at Children’s National provides funding to equip each room with an EC10, ensuring it’s always available. Additionally, the grant will support the purchase of modules to connect ventilators to the cloud, improving data capture and ensuring that important patient information is not missed.”
Not only does the technology improve patient care in real-time, but it also opens new opportunities for research and data-driven improvements.
What excites you about this?
Dr. Soghier says the ability to quickly analyze data has transformed how clinicians track patient outcomes, cutting down research time from months to weeks. This has streamlined research and made it easier to automatically track quality improvement (QI) metrics, changing the clinical environment.
The Etiometry software platform also allows us to review past data and combine it with additional patient information, enabling us to conduct studies, including a recent retrospective analysis of 879 premature babies.
“By examining oxygen treatment compliance, we found that lower compliance rates were linked to a higher likelihood of developing conditions like retinopathy of prematurity (ROP) and bronchopulmonary dysplasia (BDP), said Dr. Perazzo. “We look forward to developing new algorithms by increasing time in compliance to improve patient outcomes.”
This important research will be presented at the Pediatric Academy Society meeting later this month.