

An integrated approach to address perinatal mental health treatment
Perinatal mood and anxiety disorders (PMADs) are the most common complication of childbirth, with suicide as a leading cause of postpartum deaths.
Perinatal mood and anxiety disorders (PMADs) are the most common complication of childbirth, with suicide as a leading cause of postpartum deaths. PMADs are associated with poor maternal, infant and family outcomes. A new advocacy case study in Pediatrics led by a collaborative team of physicians at Children’s National Hospital describes the creation of the Task Force to formalize collaboration between hospital divisions, promote systems-level change and advocate for health care policy solutions.
Spearheaded by the Division of Emergency Medicine, the Goldberg Center for Community Pediatric Health and the Division of Neonatology at Children’s National, the #1 rated neonatology program in the country, the physicians who led this case study hope it can serve as a model for advocates looking to integrate PMAD screening within their own institutions. Children’s National is currently one of only a few children’s hospitals in the country that have implemented universal PMADs screening.
Lenore Jarvis, M.D., director of advocacy and health policy for the Division of Emergency Medicine at Children’s National, and Lamia Soghier, M.D., medical director of the Neonatal Intensive Care Unit (NICU) and the NICU Quality and Safety Officer at Children’s National, discussed this important work:
Q: What were you looking at with this case study?
A: Dr. Jarvis: This case study describes the implementation and outcomes of a multidisciplinary Perinatal Mental Health Task Force created at Children’s National in Washington, D.C. It was created to promote systems change and health care policy solutions for improved identification and treatment of PMADs.
Using the social-ecological model as a framework, the Task Force addressed care at the individual, interpersonal, organizational, community and policy levels. It then applied lessons learned from division-specific screening initiatives to create best practices and make hospital-wide recommendations.
This foundational work enabled us to build community bridges and break down internal barriers to shift our hospital toward prioritizing perinatal mental health. As a result, screening expanded to multiple hospital locations and the Perinatal Mental Health Screening Tool Kit was created and disseminated within the community. Task Force members also testified in governmental hearings and joined national organizations to inform policy, and Task Force and community collaborations resulted in significant grant funding.
Q: How is this work benefitting patients?
A: Dr. Soghier: Identification and early intervention for PMADs are imperative for improving health outcomes – not only for mothers but for their children and families too. Given the prevalence and negative consequences of untreated PMADs, we continue to innovate to improve the care we provide for infants and their families. We hope that this case study inspires others who value family mental health and are looking to integrate PMAD screening within their institutions.
Q: What are some of the barriers to getting this work implemented more widely?
A: Dr. Jarvis: One important thing to note is that families and medical providers alike may be unaware of how common PMADs truly are. On top of that, they’re unaware of the downstream negative impact it can have on the infant and family.
As a society, we must realize that PMADs can affect paternal caregivers. We need to have resources that also address fathers in addition to culturally and racially competent systems and resources for referral and linkage to care.
A: Dr. Soghier: Within medical systems, fragmented and siloed care delivery systems continue to be a barrier. Medical staff may also feel untrained and uncomfortable with addressing positive PMADs screens. Within the pediatric practice, differential access to services and reimbursement continue to be a concern, especially in a system where the parent is technically “not our patient.”
Identifying PMADs in our families and providing real-time resources and linkage to care has been invaluable to us. Ultimately, we seek to improve the care we provide to our infants and families and improve patient-family outcomes.
Read the full case study in the journal Pediatrics.
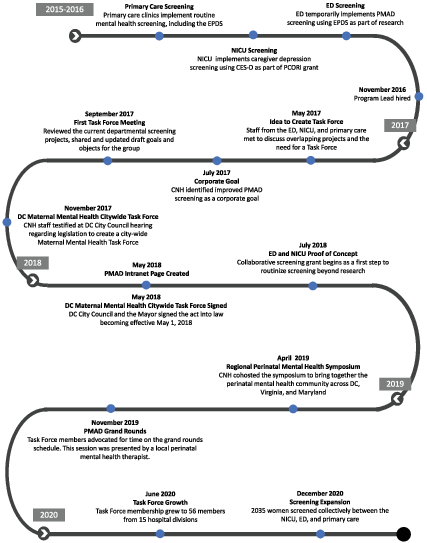
Timeline of major Task Force events. CES-D, Center for Epidemiologic Studies Depression Scale; DC, District of Columbia; PCORI, Patient-Centered Outcomes Research Institute.







