The conference offered a robust platform for presenting groundbreaking research and clinical advancements across diverse subfields such as pediatric neurology, neurosurgery, neuro-critical care, neurogenetics, neuroimmunology and neuroradiology. Esteemed medical professionals and researchers from around the world convened to share insights and innovations that are shaping the future of pediatric neurological health.
Various speakers from Children’s National led in-depth discussions on diagnostic and therapeutic innovations aimed at enhancing outcomes for children with chronic neurological and neurosurgical conditions. PNC 2024 provided an excellent platform for healthcare professionals, researchers and academics to update their knowledge and engage with leading specialists in the field.
Presenters and topics from Children’s National included:
Dana Harrar, M.D., Ph.D.: Pediatric Status Epilepticus – Monitoring and Management, Acute Stroke: Diagnosis and Critical Care Management
Daniel Donoho, M.D.: Implementing AI in the Operating Room: State of the Art and Future Directions
Tayyba Anwar, M.D.: Neonatal Encephalopathies other than HIE, Personalized Treatments for Genetic Epilepsy
Youssef Kousa, M.S., D.O., Ph.D.: Prenatal and Neonatal CNS Infections, Difficult Goals of Care and Outcome Discussions in the Neonatal ICU
The collaborative efforts with Sidra Medicine highlight a shared vision of pushing the boundaries of pediatric neurological research and treatment, ultimately aiming to improve outcomes for young patients worldwide.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/11/PNC-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-11-19 11:20:102024-11-19 11:22:10Insights and Innovations in Pediatric Neuroscience: Highlights from PNC 2024
Zika virus in blood with red blood cells, a virus which causes Zika fever found in Brazil and other tropical countries.
The National Institutes of Health (NIH) awarded Children’s National Hospital nearly $1M of research support toward uncovering the specific cellular response that happens inside a developing brain once it is infected with a virus, including how the neuron gets infected, and how it dies or survives. The research is expected to gather critical information that can inform prenatal neuro-precision therapies to prevent or attenuate the effects of endemic and pandemic viruses in the future.
“We need to use all of the information we have from ongoing and past pandemics to prevent tomorrow’s public health crisis,” said Youssef Kousa, MS, D.O., Ph.D., neonatal critical care neurologist and physician-scientist at Children’s National. “There is still here a whole lot to learn and discover. We could eventually — and this is the vision that’s inspiring us — prevent neurodevelopmental disorders before a baby is born by understanding more about the interaction between the virus, mother, fetus, and environment, among other factors.”
The clinical research findings then led to the NIH support, which then inspired more basic science research. Fast forward to now, Kousa will study how Zika affects the human brain and extrapolate what is learned and discovered for a broader understanding of neurovirology.
The research program is supported by senior scientists and advisors, including Tarik Haydar, Ph.D., and Eric Vilain, M.D., Ph.D., both at Children’s National and Avindra Nath, M.D., at NIH, as well as other leading researchers at various U.S. centers.
“This is a team effort;” added Kousa, “I’m thankful to have a group of pioneering and seasoned researchers engaged with me throughout this process to provide invaluable guidance.”
Many viruses can harm the developing brain when they replicate in the absence of host defenses, including the gene regulatory networks responsible for the neuronal response. As a result, viral infections can lead to brain injury and neurodevelopmental delays and disorders such as intellectual disability, seizures that are difficult to treat, and vision or hearing loss.
The big picture
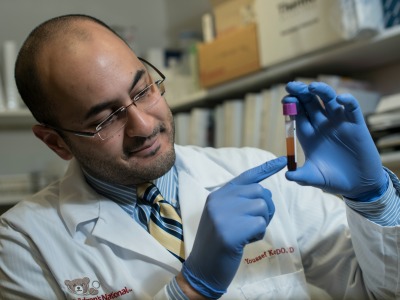
Youssef Kousa, MS, D.O., Ph.D., neonatal critical care neurologist and physician-scientist at Children’s National.
The translational research supported by NIH with this award synergistically complements nationally recognized clinical research programs and ongoing prospective cohort studies at Children’s National to identify the full spectrum of neurodevelopmental clinical outcomes after prenatal Zika and other viral infections led by Dr. Mulkey and Roberta DeBiasi, M.D., M.S..
The award also builds upon strengths at the Children’s National Research & Innovation Campus, which is in proximity to federal science agencies. Children’s National experts from the Center for Genetic Medicine Research, known for pediatric genomic and precision medicine, joined forces with the Center of Neuroscience Research and the NIH-NINDS intramural research program to focus on examining prenatal and childhood neurological disorders.
Kousa received this competitive career development award from the National Institute of Neurological Disorders and Stroke of the National Institutes of Health under Award Number K08NS119882. The research content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The hold-up in the field
Many neurodevelopmental disorders are caused by endemic viruses, such as CMV, and by viral pandemics, including rubella as seen in the 1960s and Zika since 2015. By studying Zika and other prenatal viral infections, Kousa and team hope to gain deeper biological understanding of the viral effects toward developing therapies for anticipating, treating and preventing virally induced prenatal brain injury in the long-term future.
To date, little is known about how viruses affect developing neurons and, as a result, prenatal brain injury is not yet treatable. To bridge the gap towards prenatal neuro-precision therapies, the research explores how genes regulate neuronal developmental and viral clearance by innovatively integrating three systems:
Cerebral organoids, which illuminate how a neuron reacts to a viral infection
Pre-clinical models that link prenatal brain injury to postnatal neurodevelopmental outcomes
Populational genomics to identify human genetic risk or protective factors for prenatal brain injury
Given the scope and complexity of this issue, the international Zika Genetics Consortium, founded in 2015 by Kousa and a team of leading investigators across the world, provides critical samples and resources for the third arm of the research by performing comprehensive genomic analyses using sequencing data collected from diverse human populations throughout Central and South America, which are not as heavily sequenced as Western populations. Through partnerships with the Centers for Disease Control and Prevention and NIH, the consortium’s database and biorepository houses thousands of patient records and biospecimens for research studies to better understand how viruses affect the developing human brain.
“It is inspiring to imagine that, in the longer term, we could recognize early on the level of brain-injury risk faced by a developing fetus and have the tools to mitigate ensuing complications,” said Kousa. “What is driving this research is the vision that one day, brain injury could be prevented from happening before a baby is born.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/06/zika-virus.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2022-03-15 09:34:552024-06-12 16:53:52Researcher to decipher how viruses affect the developing brain with nearly $1M NIH award
The Child Neurology Foundation has awarded Youssef A. Kousa, M.S., D.O., Ph.D., the 2020 Pediatric Epilepsy Research Foundation Shields Research Grant. The funds will support his work on identifying genetic risk factors in congenital Zika syndrome.
The Child Neurology Foundation has awarded Youssef A. Kousa, M.S., D.O., Ph.D., physician-scientist within the Division of Neurology at Children’s National Hospital, and founder and director of the Zika Genetics Consortium, the 2020 Pediatric Epilepsy Research Foundation Shields Research Grant. The funds will support his work on identifying genetic risk factors in congenital Zika syndrome.
This prestigious grant provides $100,000 of research funding to help identify treatments and cures for pediatric neurologic diseases. It will allow Dr. Kousa to test the hypothesis that rare genetic variants in individuals contributed to being affected with congenital Zika syndrome and the severity of the phenotype for those who were affected.
“Despite decades of research, identifying those at greatest risk of congenital infection or being severely affected remains an elusive goal,” says Dr. Kousa. “This research is important because identifying genetic risk or protective factors for developmental brain malformations can help teach us how the brain develops.”
In 2015, Dr. Kousa established the Zika Genetic Consortium to investigate whether maternal and fetal genetic factors can modify the risk of brain injury from congenital infections.
Dr. Kousa adds that this work will provide key insights into maternal and fetal genetic factors that can contribute to brain malformations. The hope is that these insights may one day translate into targeted prevention efforts.
“Dr. Kousa’s project is very creative and has a fantastic opportunity to look at factors of Zika on brain development,” says William D. Gaillard, M.D., division chief of both Epilepsy and Neurophysiology, and Neurology at Children’s National. “This is a very competitive award. It’s a tremendous achievement that few accomplish.”
Children’s National is the leading site for this international research study.
In 2015, Dr. Kousa established the Zika Genetic Consortium to investigate whether maternal and fetal genetic factors can modify the risk of brain injury from congenital infections. Dr. Kousa is the principal investigator of the consortium, which includes 19 co-investigators representing 13 different institutions.
The consortium is bringing together cohorts of 12,000 mother-infant participants retrospectively and prospectively. These cohorts come from 15 international health centers in seven countries in collaboration with partners at the National Institutes of Health, and the Centers for Disease Control and Prevention.
“This support gives us the opportunity to test our hypothesis,” says Dr. Kousa. “We also hope what we continue to learn about Zika can play a role in helping us understand other congenital infections and neurodevelopment diseases.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/08/Youssef-KousaImage1_-2017-updated.png400300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-08-31 15:25:302020-10-21 15:40:45Dr. Youssef Kousa awarded Pediatric Epilepsy Research Grant
Research by an international team that includes Children’s National faculty, published online Jan. 25, 2019 in Human Molecular Genetics, suggests that genetic mutations that cause cleft lip and palate also may contribute to neural tube defects, such as spina bifida.
Oral clefts are some of the most common birth defects worldwide, affecting about one in every 700 births. In the U.S., more than 4,000 babies are born each year with cleft lip, with or without cleft palate.
This defect isn’t simply a cosmetic manner: Oral clefts can severely affect feeding, speech and hearing, and they cause about 3,300 deaths annually worldwide.
To better understand these conditions, researchers have isolated a number of genetic mutations that appear to play contributing roles. These include those in a gene known as Interferon Regulatory Factor 6. New research by an international team that includes Children’s National faculty, published online Jan. 25, 2019 in Human Molecular Genetics, suggests that these mutations also may contribute to neural tube defects such as spina bifida.
In the first weeks of fetal development, the neural plate curves, creating a neural tube that, once fused shut, becomes the fetal brain and fetal spinal cord. Neural tube defects, which can range from mild to severe, are characterized by incomplete development of the brain, spinal cord or meninges. These defects can potentially result in paralysis or even fetal or neonatal demise. According to the National Institutes of Health, spina bifida, which affects the spinal cord, is the most common neural tube defect in the U.S., affecting up to 2,000 infants each year.
“Despite its high frequency, spina bifida remains among the least understood structural birth defects,” says Brian C. Schutte, an associate professor of Microbiology and Molecular Genetics, Pediatrics and Human Development at Michigan State University and the study’s senior author. “There is strong evidence that genetic factors are a leading cause of such structural birth defects, but in most cases, the cause is unknown. Our team’s study is the first published research to demonstrate that DNA variants in the gene IRF6 can cause spina bifida,” Schutte says.
What’s more, the research team identified a mechanism to explain how altering IRF6 leads to neural tube defects. This mechanism links IRF6 function to two other genes – known as transcription Factor AP2A (TFAP2A) and Grainyhead Like 3 (GRHL3) – that are also known to be required for the development of the neural tube, lip and palate.
“We’re all on the hunt for the reasons when, how and why birth defects happen,” adds Youssef A. Kousa, MS, D.O., Ph.D., a clinical fellow in the Division of Child Neurology at Children’s National Health System and the study’s lead author. “Our main goal is prevention. This paper is a significant development because our team has identified a group of genes that can potentially contribute to very common types of birth defects: craniofacial as well as neural tube defects.”
The scientific odyssey is a wonderful example of serendipity. Kousa, then working in Schutte’s lab, was studying the effects of a new mutant experimental model strain on development of the palate. But one day, he walked into Schutte’s office holding a deformed preclinical embryo and said: “Brian, look at this!”
“Weird things happen in biology,” Schutte replied and counseled him to return if it happened again. Less than two weeks later, Kousa was back with several more of the deformed preclinical embryos, saying: “OK, Brian. It happened again.”
Within hours Kousa had unearthed recently published research that included an image of a similarly affected preclinical embryo. The pair then sketched out possible intersecting genetic pathways, as they brainstormed the myriad ways to end up with that specific phenotype. Initially, they tested their hypotheses in experimental models and eventually corroborated findings through human genetic studies.
The human studies could only be performed by collaborations. Schutte shared their initial observations with human genetics researchers scattered across the country. Those labs then generously agreed to test whether DNA variants in IRF6 were associated with neural tube defects in samples from patients that they had collected over decades of research.
The team found that Tfap2a, Irf6 and Grhl3 are components of a gene regulatory network required for neurulation, a folding process that results in the neural tube bending and then fusing to become the basis of the embryo’s nervous system, from brain to spinal cord.
“Since this network is also required for formation of the lip, palate, limbs and epidermis, which develop at different times and places during embryogenesis, we suggest that the Tfap2a–Irf6–Grhl3 network is a fundamental pathway for multiple morphogenetic processes,” the researchers write.
Interferon Regulatory Factor 6 functions best when there is neither too much expression nor too little. Overexpression of Irf6 suppresses Transcription Factor Activation Protein 2A and Grainyhead Like 3, causing exencephaly, a neural tube defect characterized by the brain being located outside of the skull. Counterintuitively, experimental models that had too little Irf6 also ended up with reduced levels of Tfap2a and Grhl3 that led to a structural birth defect, but at the opposite end of the neural tube.
To test whether the experimental model findings held true in humans, they sequenced samples from people who had spina bifida and anencephaly – the rare birth defect that Kousa spotted in the experimental models – and found IRF6 function was conserved in people. Because of the genetic complexity of these birth defects, and the challenges inherent in collecting samples from cases of severe birth defects, many research teams were invited to participate in the study.
As testament to their collegiality, researchers from Stanford University, University of Texas at Austin, University of Iowa, University of Texas at Houston and Duke University agreed to share precious samples from the California Birth Defects Monitoring Program, from the Hereditary Basis of Neural Tube Defects study and from their own institutional sample collections.
“As we get better at personalized medicine, we could use this information to one day help to counsel families about their own risk and protective factors,” Kousa adds. “If we can identify the genetic pathway, we might also be able to modify it to prevent a birth defect. For example, prenatal supplementation with folic acid has led to a decrease in babies born with neural tube defects, but not all neural tube defects are sensitive to folic acid. This knowledge will help us develop individual-based interventions.”
Financial support for the research covered in this post was provided by the National Institutes of Health under grants DE13513, F31DE022696, DE025060, P01HD067244 and GM072859; startup funding from Michigan State University and the UT-Health School of Dentistry in Houston; and the Centers for Disease Control and Prevention under award number 5U01DD001033.
In addition to Kousa and Schutte, study co-authors include Huiping Zhu, Yunping Lei and Richard H. Finnell, University of Texas at Austin; Walid D. Fakhouri, University of Texas Health Science Center at Houston; Akira Kinoshita, Nagasaki University; Raeuf R. Roushangar, Nicole K. Patel, Tamer Mansour, Arianna L. Smith, and Dhruv B. Sharma, Michigan State University; A.J. Agopian and Laura E. Mitchell, University of Texas School of Public Health; Wei Yang and Gary M. Shaw, Stanford University School of Medicine; Elizabeth J. Leslie, Emory University; Xiao Li, Tamara D. Busch, Alexander G. Bassuk and Brad A. Amendt, University of Iowa; Edward B. Li and Eric C. Liao, Massachusetts General Hospital; Trevor J. Williams, University of Colorado Denver at Anschutz Medical Campus; Yang Chai, University of Southern California; and Simon Gregory and Allison Ashley-Koch, Duke University Medical Center.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/little-girl-with-spina-bifida.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-25 12:58:112024-12-30 12:46:57Oral clefts may stem from a shared genetic cause as neural tube defects
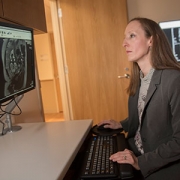
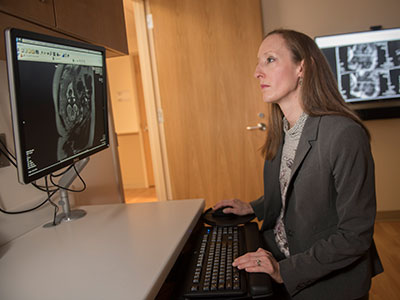
“A combination of prenatal MRI and US was able to detect Zika-related brain abnormalities during pregnancy, giving families timely information to prepare for the potential complex care needs of these infants,” says Sarah B. Mulkey, M.D., Ph.D.
Worldwide, thousands of babies have been born to mothers who were infected during pregnancy with Zika, a virus associated with neurological deficits, impaired vision and neurodevelopmental disabilities, among other birth defects. These birth defects are sometimes severe, causing lifelong disability. But they’re also relatively rare compared with the overall rates of infection.
Predicting how many Zika-exposed babies would experience neurological birth defects has been challenging.
However, an international study led by Children’s faculty suggests that ultrasound (US) imaging performed during pregnancy and after childbirth revealed most Zika-related brain abnormalities experienced by infants exposed to the Zika virus during pregnancy, according to a prospective cohort study published online Nov. 26, 2018, in JAMA Pediatrics. Some Zika-exposed infants whose imaging had been normal during pregnancy had mild brain abnormalities detected by US and magnetic resonance imaging (MRI) after they were born.
“A combination of prenatal MRI and US was able to detect Zika-related brain abnormalities during pregnancy, giving families timely information to prepare for the potential complex care needs of these infants,” says Sarah B. Mulkey, M.D., Ph.D., a fetal-neonatal neurologist at Children’s National Health System and the study’s lead author. “In our study, we detected mild brain abnormalities on postnatal neuroimaging for babies whose imaging was normal during pregnancy. Therefore, it is important for clinicians to continue to monitor brain development for Zika-exposed infants after birth.”
As of Nov. 20 2018, nearly 2,500 pregnant women in the U.S. had laboratory confirmed Zika infection, and about 2,400 of them had given birth, according to the Centers for Disease Control and Prevention (CDC). While more than 100 U.S. infants were born with Zika-associated birth defects, the vast majority of Zika-exposed U.S. infants were apparently normal at birth. The sequential neuroimaging study Dr. Mulkey leads seeks to determine the spectrum of brain findings in infants exposed to Zika in the womb using both US and MRI before and after birth.
The international research team enrolled 82 women in the study from June 15, 2016, through June 27, 2017. All of the women had been exposed to Zika during pregnancy; all but one experienced clinical symptoms by a mean gestational age of 8.2 weeks. Eighty of those women lived in or near Barranquilla, Colombia, and were exposed to Zika there. Two U.S. study participants were exposed to the primarily mosquito-borne illness during travel to Zika hot zones.
All women received fetal MRIs and US during the second and/or third trimester of pregnancy. After their infants were born, the children received brain MRI and cranial US. Blood samples from both mothers and babies were tested for Zika using polymerase chain reaction and serology.
Fetal MRI was able to discern Zika-related brain damage as early as 18 weeks gestation and picked up significant fetal brain abnormalities not fully appreciated in US imaging. In one case, the US remained normal while fetal MRI alone detected brain abnormalities. Three fetuses (4 percent) had severe fetal brain abnormalities consistent with Zika infection, including:
Two cases of heterotopias and malformations in cortical development, and
One case of parietal encephalocele, Chiari II malformation and microcephaly.
Seventy-five infants were born at term. One pregnancy was terminated at 23 weeks gestation due to the gravity of the fetal brain abnormalities. One fetus with normal imaging died during pregnancy. One newborn who was born with significant fetal brain abnormalities died at age 3 days.
Cranial US and brain MRI was performed on the majority of infants whose prenatal imaging had been normal. Seven of 53 (13 percent) Zika-exposed infants had mild brain abnormalities detected by MRI after birth. In contrast, postnatal cranial US was better at detecting changes of lenticulostriate vasculopathy, cysts within the brain’s choroid plexus (cells that produce cerebrospinal fluid), germinolytic/subependymal cysts and/or calcifications, which were seen in 21 of 57 (37 percent) infants.
“Sequential neuroimaging revealed that the majority of Zika-exposed fetuses had normal brain development. Tragically, in a small number of pregnancies, Zika-related brain abnormalities were quite severe,” Dr. Mulkey adds. “Our data support the CDC’s recommendation that cranial US be performed after Zika-exposed babies are born. In addition, there is clearly a need to follow these babies over time to gauge whether the brain anomalies we see in imaging affects language, motor and social skills.”
In addition to Dr. Mulkey, study co-authors include Dorothy I. Bulas, M.D., Gilbert Vezina, M.D., Margarita Arroyave-Wessel, MPH, Stephanie Russo, B.S, Youssef A. Kousa, D.O, Ph.D., Roberta L. DeBiasi, M.D., MS, Senior Author Adré J. du Plessis, M.B.Ch.B., MPH, all of Children’s National; Christopher Swisher, BS, Georgetown University and Caitlin Cristante, BS, Loyola University, both of whose contributions included research performed at Children’s National; Yamil Fourzali, M.D., Armando Morales, M.D., both of Sabbag Radiologos; Liliana Encinales, M.D., Allied Research Society; Nelly Pacheco, Bacteriologa, Bio-Nep; Robert S. Lanciotti, Ph.D., Arbovirus Diseases Branch, Centers for Disease Control and Prevention; and Carlos Cure, M.D., BIOMELAB.
Research reported in this news release was supported by the IKARIA fund.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/12/Sarah-B.-Mulkey.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-12-07 12:35:192024-05-29 09:02:15MRI and ultrasound imaging detect the spectrum of Zika’s impact
Like mechanics fixing a faulty engine, Youssef A. Kousa, M.S., D.O., Ph.D., says researchers will not be able to remedy problems related to IRF6, a gene implicated in cleft palate, until they better understand how the gene works.
Like all of the individual elements of fetal development, palate growth is a marvel of nature. In part of this process, ledges of tissue on the sides of the face grow downwards on each side of the tongue, then upward, fusing at the midline at the top of the mouth. The vast majority of the time, this process goes correctly. However, some part of it goes awry for the 2,650 babies born in the United States each year with cleft palates and the thousands more born worldwide with the defect.
For nearly two decades, researchers have known that a gene known as IRF6 is involved in palate formation. Studies have shown that this gene contributes about 12 percent to 18 percent of the risk of cleft palate, more than any other gene identified thus far. IRF6 is active in epithelial tissues – those that line cavities and surfaces throughout the body – including the periderm, a tissue that lines the mouth cavity and plays an important role during development.
According to Youssef A. Kousa, M.S., D.O., Ph.D., a child neurology fellow at Children’s National Health System, the periderm acts like a nonstick layer, preventing the tongue or other structures from adhering to the growing palate and preventing it from sealing at the midline. While researchers have long suspected that IRF6 plays a strong role in promoting this nonstick quality, exactly how it exerts its influence has not been clear.
“Gaining a better understanding of this gene might help us to eventually address deficits or perturbations in the system that creates the palate,” Dr. Kousa says. “Like a mechanic fixing a faulty engine, we will not be able to remedy problems related to this gene until we know how the gene works.”
“Gaining a better understanding of this gene might help us to eventually address deficits or perturbations in the system that creates the palate,” Dr. Kousa says. “Like a mechanic fixing a faulty engine, we will not be able to remedy problems related to this gene until we know how the gene works.”
In a study published July 19, 2017 by the Journal of Dental Research, Dr. Kousa and colleagues seek to decipher one piece of this puzzle by investigating how this key gene might interact with others that are active during fetal development. The researchers were particularly interested in genes that work together in a cascade of activity known as the tyrosine kinase receptor signaling pathway.
Because this pathway includes a large group of genes, Dr. Kousa and colleagues reasoned that they could answer whether IRF6 interacts with this pathway by looking at whether the gene interacts with the last member of the cascade, a gene called SPRY4. To do this, the researchers worked with experimental models that had mutations in IRF6, SPRY4 or both. If these two genes interact, the scientists hypothesized, carrying mutations in both genes at the same time should result in a dramatically different outcome compared with animals that carried mutations in just one gene.
Using selective breeding techniques, the researchers created animals that had mutations in either of these genes or in both. Their results suggest that IRF6 and SPRY4 indeed do interact: Significantly more of the oral surface was adhered to the tongue during fetal development in experimental models that had mutations in both genes compared with those that had just one single gene mutated. Examining the gene activity in the periderm cells of these affected animals, the researchers found that doubly mutated experimental models also had decreased activity in a third gene known as GRHL3, which also has been linked with cleft lip and palate.
Dr. Kousa says the research team plans to continue exploring this interaction to better understand the flow of events that lead from perturbations in these genes to formation of cleft palate. Some of the questions they would like to answer include exactly which gene or genes in the tyrosine kinase receptor signaling pathway specifically interact with IRF6 – since SPRY4 represents just the end of that pathway, others genes earlier in the pathway are probably the real culprits responsible for driving problems in palate formation. They also will need to verify if these interactions take place in humans in the same way they occur in preclinical models.
Eventually, Dr. Kousa adds, the findings could aid in personalized prenatal counseling, diagnosis and screening related to cleft palate, as well as preventing this condition during pregnancy. Someday, doctors might be able to advise couples who carry mutations in these genes about whether they are more likely to have a baby with a cleft palate or determine which select group of pregnancies need closer monitoring. Additionally, because research suggests that GRHL3 might interact with nutrients, including inositol, it might be possible to prevent some cases of cleft palate by taking additional supplements during pregnancy.
“The more we know about how these genes behave,” Dr. Kousa says, “the more we can potentially avoid fetal palate development going down the wrong path.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/07/Cleft-Palate-Baby.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-07-19 12:13:062024-06-05 11:24:28Understanding genetic synergy in cleft palate
A research team that includes Youssef A. Kousa, M.S., D.O., Ph.D., has created a novel tool to delete Interferon regulatory factor 6, which regulates how epidermal cells differentiate, multiply and migrate.
A research team has created a novel tool to delete Interferon regulatory factor 6 (Irf6), which regulates how epidermal cells differentiate, multiply and migrate.
Mutations of this critical transcription factor are implicated in two orofacial clefting disorders. As with other transcription factors, the IRF6 protein binds to specific regions of DNA and plays a role in that specific gene’s activity. With van der Woude syndrome, a rare disease that occurs in 1 in 35,000 individuals, the National Institutes of Health (NIH) says mutations to the IRF6 gene inhibit production of the IRF6 protein. That protein shortfall lies at the heart of incomplete development and stalled maturation of tissues in the skull and face. For popliteal pterygium syndrome, IRF6 mutations can trigger facial abnormalities, webbed skin, and fused fingers and toes.
According to the NIH, the IRF6 protein is active in embryonic skin cells that later become tissue in the head, face and tongue. The study authors write that DNA variation in the IRF6 gene (which issues the marching orders to make the IRF6 protein) significantly heightens risk for developing non-syndromic cleft lip and palate, one of the most common congenital defects.
Studying the function of this critical gene in preclinical models has been hobbled by the fact that experimental models created without the Irf6 allele are born with severe skin, limb and craniofacial defects and die shortly after birth.
To overcome this hurdle, the research team did a bit of creative genetic shuffling to make a conditional allele of Irf6 to test in specific tissues at specific times as the experimental animals matured.
“The experimental models with the Irf6 conditional allele were viable after birth and, in fact, showed no developmental or reproductive defects when compared with their litter mates – which provides a reassurance that this specific change does not appear to affect overall normal gene function,” says Youssef A. Kousa, M.S., D.O., Ph.D., a pediatric resident in the child neurology track at Children’s National Health System and co-lead author of the technology report published online May 8, 2017 in Genesis.
To drill down into how the conditional allele affected the experimental models, the research team bred them with other animals specially designed to illuminate the function of the conditional allele. Some genotypes were lost, as was expected. Litters that were hypothesized to experience certain rates of severe limb, skin and craniofacial abnormalities did so. Immunostaining revealed IRF6 expression throughout the spinous layer and basal – or deepest – layer of the epidermis, but such expression was lacking in wildtype and knockout embryos.
In a different group of experimental models, the researchers added the deleter strain Ella-Cre. Nineteen resulting embryos were positive for the conditional allele but showed no evidence of recombination. Eight normal embryos showed incomplete recombination. Nine embryos showed complete recombination in tail tissue. Just one embryo phenocopied the wild type embryos.
“Our research team successfully created the conditional allele for IRF6, which will open the door to future studies of gene function in neonatal experimental models,” Dr. Kousa and colleagues conclude. “Even though the allele is capable of recombination, we saw that efficacy varied and is linked to specific cell types. One possible explanation is variation in chromatin structure at the IRF6 locus.”
Future research will explore the utility of other Cre-drivers, such as Gdf9-Cre or CAG-Cre, to provide additional clarity about the functionality of the newly derived conditional alleles.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/06/Youssef-A.-Kousa.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-06-20 13:01:342017-07-19 12:17:22Generating a conditional allele of Irf6
An international study that includes Sarah B. Mulkey, M.D., Ph.D., aims to answer one of the most vexing questions about Zika: If babies’ brains appear “normal” at birth, have they survived Zika exposure in the womb with few neurological repercussions? Dr. Mulkey presented preliminary findings at PAS2017.
It has been well established by researchers, including scientists at Children’s National Health System, that the Zika virus is responsible for a slew of birth defects – such as microcephaly, other brain malformations and retinal damage – in babies of infected mothers. But how the virus causes these often devastating effects, and who exactly is affected, has not been explained fully.
Also unknown is whether exposed babies that appear normal at birth are truly unaffected by the virus or have hidden problems that might surface later. The majority of babies born to Zika-infected mothers in the United States appear to have no evidence of Zika-caused birth defects, but that’s no guarantee that the virus has not caused lingering damage.
Recently, Sarah B. Mulkey, M.D., Ph.D., made a trip to Colombia, where Children’s National researchers are collaborating on a clinical study. There, she tested Zika-affected babies’ motor skills as they sat, stood and lay facing upward and downward. The international study aims to answer one of the most vexing questions about Zika: If babies’ brains appear “normal” at birth, have they survived Zika exposure in the womb with few neurological repercussions?
“We don’t know the long-term neurological consequences of having Zika if your brain looks normal,” says Dr. Mulkey, a fetal-neonatal neurologist who is a member of Children’s Congenital Zika Virus Program. “That is what’s so scary, the uncertainty about long-term outcomes.”
According to the Centers for Disease Control and Prevention (CDC), one in 10 pregnancies across the United States with laboratory-confirmed Zika virus infection results in birth defects in the fetus or infant. For the lion’s share of Zika-affected pregnancies, then, babies’ long-term prospects remain a mystery.
“This is a huge number of children to be impacted and the impact, as we understand, has the potential to be pretty significant,” Dr. Mulkey adds.
Dr. Mulkey, the lead author, presented the research group’s preliminary findings during the 2017 annual meeting of the Pediatric Academic Societies (PAS). The presentation was one of several that focused on the Zika virus. Roberta L. DeBiasi, M.D., M.S., chief of the Division of Pediatric Infectious Diseases at Children’s National, organized two invited symposia devoted to the topic of Zika: Clinical perspectives and knowledge gaps; and the science of Zika, including experimental models of disease and vaccines. Dr. DeBiasi’s presentation included an overview of the 68 Zika-exposed or infected women and infants seen thus far by Children’s multidisciplinary Congenital Zika Virus Program.
“As the world’s largest pediatric research meeting, PAS2017 is an ideal setting for panelists to provide comprehensive epidemiologic and clinical updates about the emergence of Congenital Zika Syndrome and to review the pathogenesis of infection as it relates to the fetal brain,” Dr. DeBiasi says. “With temperatures already rising to levels that support spread of the Aedes mosquito, it is imperative for pediatricians around the world to share the latest research findings to identify the most effective interventions.”
As one example, Dr. Mulkey’s research sought to evaluate the utility of using magnetic resonance imaging (MRI) to evaluate fetal brain abnormalities in 48 babies whose mothers had confirmed Zika infection during pregnancy. Forty-six of the women/infant pairs enrolled in the prospective study are Colombian, and two are Washington, D.C. women who were exposed during travel to a Zika hot zone.
The women were infected with Zika during all three trimesters and experienced symptoms at a mean gestational age of 8.4 weeks. The first fetal MRIs were performed as early as 18 weeks’ gestation. Depending upon the gestational age when they were enrolled in the study, the participants had at least one fetal MRI as well as serial ultrasounds. Thirty-six fetuses had a second fetal MRI at about 31.1 gestational weeks. An experienced pediatric neuroradiologist evaluated the images.
Among the 48 study participants, 45 had “normal” fetal MRIs.
Three fetuses exposed to Zika in the first or second trimester had abnormal fetal MRIs:
One had heterotopia and an early, abnormal fold on the surface of the brain, indications that neurons did not migrate to their anticipated destination during brain development. This pregnancy was terminated at 23.9 gestational weeks.
One had parietal encephalocele, a rare birth defect that results in a sac-like protrusion of the brain through an opening in the skull. According to the CDC, this defect affects one in 12,200 births, or 340 babies, per year. It is not known if this rare finding is related to Zika infection.
One had a thin corpus callosum, dysplastic brainstem, heterotopias, significant ventriculomegaly and generalized cerebral/cerebellar atrophy.
“Fetal brain MRI detected early structural brain changes in fetuses exposed to the Zika virus in the first and second trimester,” Dr. Mulkey says. “The vast majority of fetuses exposed to Zika in our study had normal fetal MRI, however. Our ongoing study, underwritten by the Thrasher Research Fund, will evaluate their long-term neurodevelopment.”
Adré J. du Plessis, MB.Ch.B., M.P.H., director of the Fetal Medicine Institute and senior author of the paper, notes that this group “is a very important cohort to follow as long as Dr. Mulkey’s funding permits. We know that microcephaly is among the more devastating side effects caused by Zika exposure in utero. Unanswered questions remain about Zika’s impact on hearing, vision and cognition for a larger group of infants. Definitive answers only will come with long-term follow-up.”
Many of the Colombian families live in Sabanalarga, a relatively rural, impoverished area with frequent rain, leaving pockets of fresh water puddles that the mosquito that spreads Zika prefers, Dr. Mulkey adds. Families rode buses for hours for access to fetal MRI technology, which is not common in Colombia.
“The mothers are worried about their babies. They want to know if their babies are doing OK,” she says.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/05/Sarah-Mulkey-Columbia-Zika-Study.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-05-22 15:19:372024-06-05 11:24:44Damage may lurk in “normal” Zika-exposed brains
A multidisciplinary team at Children’s National has consulted on 66 Zika-affected pregnancies and births since May 2016.
The first pregnant patient with worries about a possible Zika virus infection arrived at the Children’s National Health System Fetal Medicine Institute on Jan. 26, 2016, shortly after returning from international travel.
Sixteen months ago, the world was just beginning to learn how devastating the mosquito-borne illness could be to fetuses developing in utero. As the epidemic spread, a growing number of sun-splashed regions that harbor mosquitoes that efficiently spread the virus experienced a ballooning number of Zika-affected pregnancies and began to record sobering birth defects.
The Washington, D.C. patient’s concerns were well-founded. Exposure to Zika virus early in her pregnancy led to significant fetal brain abnormalities, and Zika virus lingered in the woman’s bloodstream months after the initial exposure — longer than the Centers for Disease Control and Prevention (CDC) then thought was possible.
In the intervening months, a multidisciplinary team at Children National has consulted on 66 pregnancies and infants with confirmed or suspected Zika exposure. Thirty-five of the Zika-related evaluations were prenatal, and 31 postnatal evaluations assessed the impact of in utero Zika exposure after the babies were born.
The continuum of Zika-related injuries includes tragedies, such as a 28-year-old pregnant woman who was referred to Children’s National after imaging hinted at microcephaly. Follow-up with sharper magnetic resonance imaging (MRI) identified severe diffuse thinning of the cerebral cortical mantle, evidence of parenchymal cysts in the white matter and multiple contractures of upper and lower extremities with muscular atrophy.
According to a registry of Zika-affected pregnancies maintained by the CDC, one in 10 pregnancies across the United States with laboratory-confirmed Zika virus infection has resulted in birth defects in the fetus or infant.
“More surprising than that percentage is the fact that just 25 percent of infants underwent neuroimaging after birth – despite the CDC’s recommendation that all Zika-exposed infants undergo postnatal imaging,” says Roberta L. DeBiasi, M.D., M.S., chief of the Division of Pediatric Infectious Diseases and co-director of the Congenital Zika Virus Program at Children’s National. “Clinicians should follow the CDC’s guidance to the letter, asking women about possible exposure to Zika and providing multidisciplinary care to babies after birth. Imaging is an essential tool to accurately monitor the growing baby’s brain development.”
Adré du Plessis, M.B.Ch.B., M.P.H., director of the Fetal Medicine Institute and Congenital Zika Virus Program co-leader, explains the challenges: ”When it comes to understanding the long-term consequences for fetuses exposed to the Zika virus, we are still on the steepest part of the learning curve. Identifying those children at risk for adverse outcomes will require a sustained and concerted multidisciplinary effort from conception well beyond childhood.”
In addition to counseling families in the greater Washington, D.C. region, the Children’s research team is collaborating with international colleagues to conduct a clinical trial that has been recruiting Zika-infected women and their babies in Colombia. Pediatric Resident Youssef A. Kousa, D.O., Ph.D., M.S., and Neurologist Sarah B. Mulkey, M.D., Ph.D., will present preliminary findings during Research and Education Week 2017.
In Colombia as well as the District of Columbia, a growing challenge continues to be assessing Zika’s more subtle effects on pregnancies, developing fetuses and infants, says Radiologist Dorothy Bulas, M.D., another member of Children’s multidisciplinary Congenital Zika Virus Program.
The most severe cases from Brazil were characterized by interrupted fetal brain development, smaller-than-normal infant head circumference, brain calcifications, enlarged ventricles, seizures and limbs folded at odd angles. In the United States and many other Zika-affected regions, Zika-affected cases with such severe birth defects are outnumbered by infants who were exposed to Zika in utero but have imaging that appears normal.
In a darkened room, Dr. Bulas pores over magnified images of the brains of Zika-infected babies, looking for subtle differences in structure that may portend future problems.
“There are some questions we have answered in the past year, but a number of questions remain unanswered,” Dr. Bulas says. “For neonates, that whole area needs assessment. As the fetal brain is developing, the Zika virus seems to affect the progenitor cells. They’re getting hit quite early on. While we may not detect brain damage during the prenatal period, it may appear in postnatal images. And mild side effects that may not be as obvious early on still have the potential to be devastating.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/08/DeBiasi-and-du-Plessis.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-04-21 11:07:442019-03-11 10:00:24Zika virus, one year later
Youssef A. Kousa, D.O., Ph.D., M.S., is examining whether interplays between certain genes make some women more vulnerable to symptomatic Zika infections.
A Maryland woman traveled to the Dominican Republic early in her pregnancy, spending three weeks with family. She felt dizzy and tired and, at first, attributed the lethargy to jet lag. Then, she experienced a rash that lasted about four days. She never saw a bite or slapped a mosquito while in the Dominican Republic but, having heard about the Zika virus, asked to be tested.
Her blood tested positive for Zika.
Why was this pregnant woman infected by Zika while others who live year-round in Zika hot zones remain free of the infectious disease? And why was she among the slim minority of Zika-positive people to show symptoms?
Youssef A. Kousa, D.O., Ph.D., M.S., a pediatric resident in the child neurology track at Children’s National Health System, is working on a research study that will examine whether interplays between certain genes make some women more vulnerable to symptomatic Zika infections during pregnancy, leaving some fetuses at higher risk of developing microcephaly.
Dr. Kousa will present preliminary findings during Research and Education Week 2017 at Children’s National.
At sites in Puerto Rico, Colombia and Washington D.C., Dr. Kousa and his research collaborators are actively recruiting study participants and drawing blood from women whose Zika infections were confirmed in the first or second trimester of pregnancy. The blood is stored in test tubes with purple caps, a visual cue that the tube contains an additive that binds DNA, preventing it from being cut up. Additional research sites are currently being developed.
When the blood arrives at Children’s National, Dr. Kousa will use a centrifuge located in a sample preparation room to spin the samples at high speed for 11 minutes. The sample emerges from the centrifuge in three discrete layers, separated by weight. The rose-colored section that rises to the top is plasma. Plasma contains tell-tale signs of the immune system’s past battles with viruses and will be analyzed by Roberta L. DeBiasi, M.D., M.S., Chief of the Division of Pediatric Infectious Diseases at Children’s National, and Dr. Kousa’s mentor.
A slender line at the middle indicates white blood cells. The dark red layer is heavier red blood cells that sink to the bottom. This bottom half of the test tube, where the DNA resides, is where Dr. Kousa will perform his genetic research.
For years, Dr. Kousa has worked to identify genetic risk factors that influence which fetuses develop cleft lip and palate. In addition to genetic variances that drive disease, he looks at environmental overlays that can trigger genes to respond in ways that cause pediatric disease. When Zika infections raced across the globe, he says it was important to apply the same genetic analyses to the emerging disease. Genes make proteins that carry out instructions, but viral infection disrupts how genes interact, he says. Cells die. Other cells do not fully mature.
While certain poverty-stricken regions of Brazil have recorded the highest spikes in rates of microcephaly, more is at play than socioeconomics, he says. “It didn’t feel like all of the answers lie in the neighborhood. One woman with a Zika-affected child can live just down the street from a child who is more or less severely affected by Zika.”
As a father, Dr. Kousa is particularly concerned about how Zika stunts growth of the fetal brain at a time when it should expand exponentially. “I have three kids. You see them as they achieve milestones over time. It makes you happy and proud as a parent,” he says.
Sarah B. Mulkey, M.D., Ph.D., is studying whether infants exposed to Zika in utero achieve the same developmental milestones as uninfected infants.
While Dr. Kousa concentrates on Zika’s most devastating side effects, his colleague Sarah B. Mulkey, M.D., Ph.D., is exploring more subtle damage Zika can cause to fetuses exposed in utero. In the cohort of Colombian patients that Dr. Mulkey is researching, just 8 percent had abnormal fetal brain magnetic resonance images (MRIs). At first glance, the uncomplicated MRIs appear to be reassuring news for the vast majority of pregnant women.
Dr. Mulkey also will present preliminary findings during Research and Education Week 2017 at Children’s National.
In the fetus, the Zika virus makes a beeline to the developing brain where it replicates with ease and can linger after birth. “We need to be cautious about saying the fetal MRI is ‘normal’ and the infant is going to be ‘normal,’ ” Dr. Mulkey says. “We know with congenital cytomegalovirus that infected infants may not show symptoms at birth yet suffer long-term consequences, such as hearing deficits and vision loss.”
Among Zika-affected pregnancies in Colombia in which late-gestational age fetal MRIs were normal, Dr. Mulkey will use two different evaluation tools at 6 months and 1 year of age to gauge whether the babies accomplish the same milestones as peers. One evaluation tool is a questionnaire that has been validated in Spanish.
At 6 months and 1 year of age, the infants’ motor skills will be assessed, such as their ability to roll over in both directions, sit up, draw their feet toward their waist, stand, take steps independently and purposefully move their hands. Videotapes of the infants performing the motor skills will be scored by Dr. Mulkey and her mentor, Adre du Plessis, M.B.Ch.B., Chief of the Division of Fetal and Transitional Medicine at Children’s National. The Thrasher Research Fund is funding the project, “Neurologic outcomes of apparently normal newborns from Zika virus-positive pregnancies,” as part of its Early Career Award Program.
Both research projects are extensions of a larger multinational study co-led by Drs. du Plessis and DeBiasi that explores the impact of prolonged Zika viremia in pregnant women, fetuses and infants; the feasibility of using fetal MRI to describe the continuum of neurological impacts in Zika-affected pregnancies; and long-term developmental issues experienced by Zika-affected infants.
Children’s National research scientists are working to unravel the complicated web of genetic interactions that lead children to develop cleft lip and palate.
On June 26, 2000, scientists around the world hailed the first draft of the human genetic code as a scientific milestone that eventually would revolutionize the practice of medicine. By knowing the approximately 20,000 protein-coding genes for humans, many speculated that researchers and doctors eventually might elucidate the unique factors that influence thousands of diseases—and, someday, make it easier to find custom ways to treat these conditions.
“It is humbling for me and awe inspiring to realize that we have caught the first glimpse of our own instruction book, previously known only to God,” said Francis S. Collins, M.D., Ph.D., who directed the international effort to sequence the human genome and who now directs the National Institutes of Health.
Nearly two decades later, actually using this wealth of information has proven exceedingly more complicated than many envisioned. While some genetic diseases like Huntington’s disease or sickle cell anemia follow a simple pattern in which variations in a single gene lead to deleterious effects, the vast majority of other genetic health problems result from the interaction of multiple genes, from a handful to hundreds.
One condition that has proven especially tricky to understand on the genetic level is cleft lip and palate (CLP), says Youssef A. Kousa, D.O., Ph.D., a pediatric neurology resident at Children’s National Health System who has made human development a central focus of his research program. CLP, which affects about 1 in 1,000 babies born worldwide, can be devastating, Kousa explains. At some point between 6 and 12 weeks gestation, the palate and lip fail to close in some fetuses. Those children are born with a fissure that can significantly impair eating and speaking and that can complicate social interactions.
While researchers have linked some genes to CLP, Kousa says it has become increasingly clear that these genes do not exert their influence in isolation. In a review paper published recently in Developmental Dynamics, he and Brian C. Schutte, Ph.D., of Michigan State University, detail the story of three of those genes. The trio plays a role in CLP but also is implicated in another devastating congenital problem, neural tube defects.
One of these genes is IRF6, which scientists tagged as the gene responsible for inherited forms of CLP called van der Woude syndrome and popliteal pterygium syndrome more than a decade ago. In the interim, research has shown IRF6 also appears to be important in orofacial clefting that occurs independently of these syndromes. Estimates suggest that mutations in IRF6 increase the risk for CLP by 12 percent to 18 percent.
That means at least 80 percent of the risk for clefting is caused by different genes. Kousa and Schutte write that one of these is GRHL3, which also can cause van der Woude syndrome if it is mutated. GRHL3 is regulated by IRF6, Kousa explains. So, if IRF6 does not work properly, neither does GRHL3.
But what regulates IRF6? Upstream of this important gene is another called TFAP2A. The healthy operation of TFAP2A is key for IRF6 and orofacial clefting. Complicating the scenario further, several studies also have shown that TFAP2A is essential for normal development of the palate and neural tube, the embryo’s precursor to the central nervous system that eventually develops into the brain and spinal cord.
To shed light on the interplay of the full array of genes involved CLP, Kousa and colleagues recently published a paper in Birth Defects Research in which they use computer programs to analyze datasets on all genes identified thus far that are involved in orofacial and neural tube development and which molecules these genes produce and target. Their analyses showed that many of these genes are linked in associated pathways that influence vast realms of development, risk of cancer and folate metabolism. (Women who take folic acid supplements before getting pregnant and during pregnancy can reduce birth defect risks.)
By better understanding how these genes are connected into networks, Kousa says, researchers may be able to reduce the risk of both CLP and neural tube defects with a single intervention. However, like the study of genetic diseases itself, finding the right intervention might not be so simple. A drug or supplement that can alleviate one condition might exacerbate others, based on the complicated web of genetic interactions, he says.
“That’s why work from our lab and others is so important,” Kousa says. “It adds layers and layers of knowledge that, eventually, we’ll be able to put together to help prevent these devastating problems.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/12/Cleft-Lip-Homepage.jpg334500Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-12-15 15:07:362017-06-20 13:04:00Cleft lip and palate: caught in the web of genetic interactions