Fighting lethal cancer with a one-two punch
The immune system is the ultimate yin and yang, explains Anthony D. Sandler, M.D., senior vice president and surgeon-in-chief of the Joseph E. Robert Jr. Center for Surgical Care at Children’s National in Washington, D.C. With an ineffective immune system, infections such as the flu or diarrheal illness can run unchecked, causing devastating destruction. But on the other hand, excess immune activity leads to autoimmune diseases, such as lupus or multiple sclerosis. Thus, the immune system has “checks and balances” to stay controlled.
Cancer takes advantage of “the checks and balances,” harnessing the natural brakes that the immune system puts in place to avoid overactivity. As the cancer advances, molecular signals from tumor cells themselves turn on these natural checkpoints, allowing cancers to evade immune attack.
Several years ago, a breakthrough in pharmaceutical science led to a new class of drugs called checkpoint inhibitors. These medicines take those proverbial brakes off the immune system, allowing it to vigorously attack malignancies. However, Dr. Sandler says, these drugs have not worked uniformly and in some cancers, they barely work at all against the cancer.
One of these non-responders is high risk neuroblastoma, a common solid tumor found outside the skull in children. About 800 U.S. children are diagnosed with this cancer every year. And kids who have the high-risk form of neuroblastoma have poor prognoses, regardless of which treatments doctors use.
However, new research could lead to promising ways to fight high-risk neuroblastoma by enabling the immune system to recognize these tumors and spark an immune response. Dr. Sandler and colleagues recently reported on these results in the Jan. 29, 2018, PLOS Medicine using an experimental model of the disease.
The researchers created this model by injecting the preclinical models with cancer cells from an experimental version of neuroblastoma. The researchers then waited several days for the tumors to grow. Samples of these tumors showed that they expressed a protein on their cell surfaces known as PD-L1, a protein that is also expressed in many other types of human cancers to evade immune system detection.
To thwart this protective feature, the researchers made a cancer vaccine by removing cells from the experimental model’s tumors and selectively turning off a gene known as Id2. Then, they irradiated them, a treatment that made these cells visible to the immune system but blocked the cells from dividing to avoid new tumors from developing.
They delivered these cells back to the experimental models, along with two different checkpoint inhibitor drugs – antibodies for proteins known as CLTA-4 and PD-L1 – over the course of three treatments, delivered every three days. Although most checkpoint inhibitors are administered over months to years, this treatment was short-term for the experimental models, Dr. Sandler explains. The preclinical models were completely finished with cancer treatment after just three doses.
Over the next few weeks, the researchers witnessed an astounding turnaround: While experimental models that hadn’t received any treatment uniformly died within 20 days, those that received the combined vaccine and checkpoint inhibitors were all cured of their disease. Furthermore, when the researchers challenged these preclinical models with new cancer cells six months later, no new tumors developed. In essence, Dr. Sandler says, the preclinical models had become immune to neuroblastoma.
Further studies on human patient tumors suggest that this could prove to be a promising treatment for children with high-risk neuroblastoma. The patient samples examined show that while tumors with a low risk profile are typically infiltrated with numerous immune cells, tumors that are high-risk are generally barren of immune cells. That means they’re unlikely to respond to checkpoint inhibiting drugs alone, which require a significant immune presence in the tumor microenvironment. However, Dr. Sandler says, activating an immune response with a custom-made vaccine from tumor cells could spur the immune response necessary to make these stubborn cancers respond to checkpoint inhibitors.
Dr. Sandler cautions that the exact vaccine treatment used in the study won’t be feasible for people. The protocol to make the tumor cells immunogenic is cumbersome and may not be applicable to gene targeting in human patients. However, he and his team are currently working on developing more feasible methods for crafting cancer vaccines for kids. They also have discovered a new immune checkpoint molecule that could make this approach even more effective.
“By letting immune cells do all the work we may eventually be able to provide hope for patients where there was little before,” Dr. Sandler says.
In addition to Dr. Sandler, study co-authors include Priya Srinivasan, Xiaofang Wu, Mousumi Basu and Christopher Rossi, all of the Joseph E. Robert Jr. Center for Surgical Care and The Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI), at Children’s National in Washington, D.C.
Financial support for research described in this post was provided by the EVAN Foundation, the Catherine Blair foundation, the Michael Sandler Research Fund and SZI.
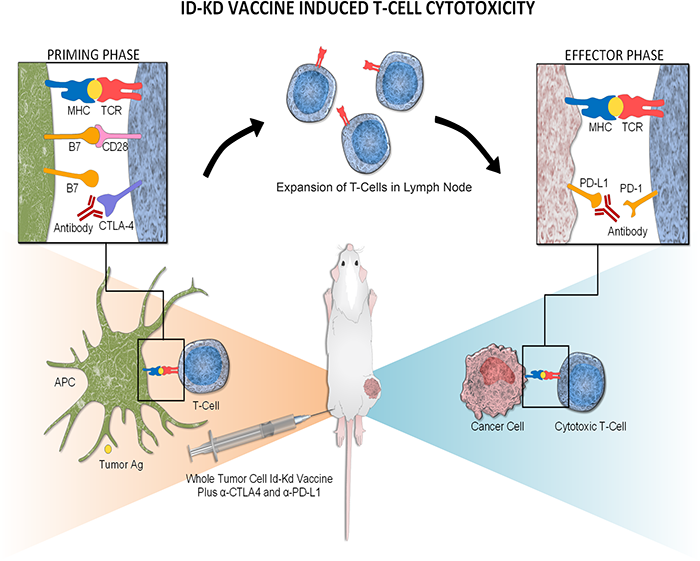
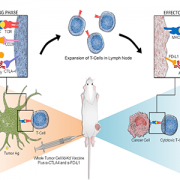
Mechanism of Id2kd Neuro2a vaccination combined with α-CTLA-4 and α-PD-L1 immunotherapy in a neuroblastoma model. During a vaccine priming phase, CTLA-4 blockade enhances activation and proliferation of T-cells that express programmed cell death 1 (PD1) and migrate to the tumor. Programmed cell death-ligand 1 (PD-L1) is up-regulated on the tumor cells, inducing adaptive resistance. Blocking PD-L1 allows for enhanced cytotoxic effector function of the CD8+ tumor-infiltrating lymphocytes. Artist: Olivia Abbate