Clinical Trial Spotlight: Treating tumors with ThermoDox® and MR-HIFU
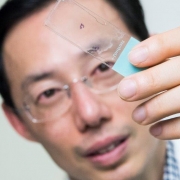
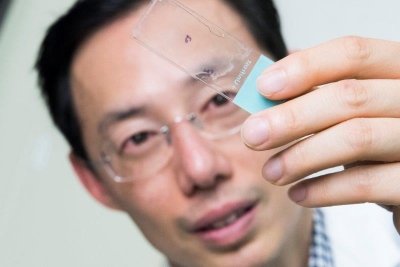
Karun Sharma, M.D., is working with AeRang Kim, M.D., Ph.D., to evaluate the use of ThermoDox®, a heat-activated chemotherapy drug, in combination with noninvasive magnetic resonance-guided high-intensity focused ultrasound (MR-HIFU) to treat refractory or relapsed solid tumors in children and young adults.
A Phase I Study of Lyso-thermosensitive Liposomal Doxorubicin (LTLD, ThermoDox®) and Magnetic Resonance-Guided High Intensity Focused Ultrasound for Relapsed or Refractory Solid Tumors in Children, Adolescents, and Young Adults.
- PI: AeRang Kim, M.D., Ph.D.
- Status: Currently enrolling
- Sponsor: Children’s Research Institute
This study is looking to determine the maximum tolerated dose (MTD) and recommended phase 2 dose (RP2D) of lyso-thermosensitive liposomal doxorubicin (LTLD), a heat-activated formulation of liposomal doxorubicin with unique property of heat-activated release of doxorubicin, administered in combination with magnetic resonance-guided high-intensity focused ultrasound (MR-HIFU) in children with relapsed/refractory solid tumors.
MR-HIFU is an innovative device that provides precise and controlled delivery of heat inside a tumor using an external applicator. Unlike other heating systems used in local therapy, MR-HIFU is entirely non-invasive and does not use any radiation. Integration of MR imaging allows for real-time temperature monitoring for accurate and precise targeting of tumors. LTLD is a novel formulation of doxorubicin with the unique property of heat-activated release. This selective drug delivery mechanism allows for local and rapid release of doxorubicin in high concentrations in tumors when heated. This novel combination may potentiate known effective therapy to improve local control and drug delivery without increasing toxicity.
Children’s National Health System and Celsion Corp, a leading oncology drug-development company, were the first to launch a clinical study in the U.S. that evaluates the use of ThermoDox® with MR-HIFU. Learn more about the clinical trial.
For more information about this trial or other trials available at Children’s National, contact:
Melissa Salerno
Clinical Research Program Manager
202-476-2142
msalerno@childrensnational.org
View more open phase 1 and phase 2 cancer clinical trials at Children’s National.
The Children’s National Center for Cancer and Blood Disorders is committed to providing the best care for pediatric patients. Our experts play an active role in innovative clinical trials to advance pediatric cancer care. We offer access to novel trials and therapies, some of which are only available here at Children’s National. With research interests covering nearly aspect of pediatric cancer care, our work is making great advancements in childhood cancer.