Real-time surgical guidance system enables multimodal tissue monitoring
For the first time, researchers at Children’s National Hospital successfully demonstrated a label-free tissue perfusion imaging in a pre-clinical model, according to a study published in IEEE Transactions on Biomedical Engineering.
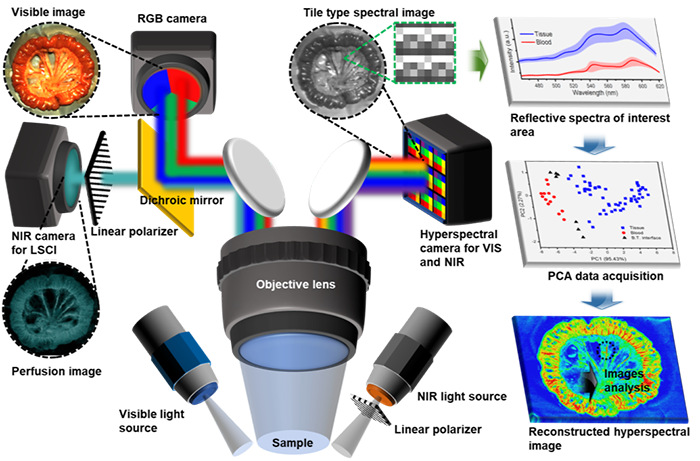
Richard Jaepyeong Cha, Ph.D., research faculty associate professor at Children’s National, and colleagues combined visible, near-infrared laser speckle contrast imaging (LSCI) and snapshot hyperspectral (HSI) cameras into a single clinical multimodal imaging device suitable for real-time intraoperative visualization and demonstrated such a device in a surgical model for the first time, to the best knowledge of the authors. This system provides instant microcirculation information about the ischemic regions, normal tissue and transitional ischemic zones with quantitative values that are reproducible.
“Our pre-clinical work demonstrated a novel, dye-free imaging platform for quantitatively assessing bowel perfusion. The ability to identify optimal surgical resection margins can improve surgical performance and patient outcome in terms of more targeted bowel resection and bowel preservation without anastomotic leakage,” Cha said. “This new optical imaging and quantitative assessment technology holds great promise to solving the long-standing issue of suboptimal assessment of intestinal viability.”
Intraoperative imaging techniques for the precise monitoring of blood flow, hemorrhage and oxygen saturation are needed to minimize errors caused by blood vessel ligation to reduce surgical blood loss and successfully isolate and resect ischemic regions.
When the blood flow, hemorrhage and oxygen are not monitored properly, anastomotic leak (AL) is a serious complication of intestinal surgery that can occur due to a technical error, and most frequently because of poorly vascularized intestine.
This complication of intestinal surgery carries with it a reported mortality ranging from 6 to 39%. The best time to prevent a possible AL is during its creation in the operating room.
Creating a healthy and safe intestinal anastomosis requires a good blood supply to the two ends of bowel to be joined. The tools for diagnosing well-perfused bowel intraoperatively are limited and often rely on the subjective evaluation of the surgeon.
“We are hoping that the use and application of multimodal LSCI/HSI imaging, capable of both non-invasive and quantitative gross tissue perfusion assessment, will provide colorectal/general surgeons with a convenient and objective method for assessment of bowel perfusion characteristics and facilitate surgical transection in tissues requiring colorectal anastomosis,” Cha said.
Recently, indocyanine green fluorescence angiography (ICG-FA) was introduced for intraoperative assessment of anastomotic perfusion. Preliminary evidence suggests that ICG-FA may reduce the rate of anastomotic leakage in gastrointestinal surgery.
Perfusion assessment at the site of anastomosis may alter surgical strategy and possibly reduce anastomotic leakage rates. However, ICG-FA evaluation requires an exogenous fluorophore and the surgeon must subjectively assess the quality of perfusion. For an ideal intestinal viability test, it is essential that the technique is easily performed by the surgeon, minimally invasive, objective and reproducible—which is what Lee et al. demonstrate with their new approach.