Pediatric solid tumors like neuroblastoma remain a major cause of illness and death, because traditional treatments effective for other tumor types have had only limited success.
A novel immunotherapy approach that involves training autologous T cells derived from peripheral blood mononuclear cells (PBMCs) has shown early signs of safety and efficacy in a small pre-clinical model. The approach, pioneered by researchers within the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital, may have future implications for the treatment of intractable pediatric solid tumors such as neuroblastoma.
What it means
Pediatric solid tumors like neuroblastoma remain a major cause of illness and death, because traditional treatments effective for other tumor types have had only limited success. There is an urgent need for innovative strategies to effectively target these tumors.
This study presents another approach to cell therapy that collects peripheral blood mononuclear cells from the patient and teaches them to target and eliminate solid tumor cells through exposure to similar tumor cells in a controlled laboratory setting. The cells are then primed to find and attack the solid tumor cells when reintroduced, an approach known as adoptive immunotherapy.
What’s new
The authors note that more well-established modalities such as CAR-T and TCR-T therapies have also made significant advances and demonstrate clinical promise at battling cancers such as neuroblastoma. However, the approach presented in the paper offers early promise of an additional potential strategy, especially in a context “where simplicity, speed and safety are priorities.”
By using small molecule treatments, the authors induce an immunogenic response in neuroblastoma tumor cells, making them more recognizable and attackable by immune cells. Ex vivo training of PBMCs with treated neuroblastoma cells exhibited strong tumor-killing activity.
The authors highlight a few key differences of this approach versus existing adoptive cellular therapies. The method “is technically straightforward, requiring only small tumor samples and peripheral blood mononuclear cells (PBMCs), and avoids the need for the complex genetic engineering intrinsic to CAR-T and TCR-T manufacturing,” the authors write. This method leverages ex vivo tumor cell modification, which may mitigate systemic toxicities. “Additionally, because our approach is not limited to a few surface antigens, it may expand the repertoire of actionable tumor-associated targets.”
Children’s National leads the way
Children’s National is a leader in the development of cell therapies for a wide range of pediatric conditions, including pediatric cancer, HIV/AIDS, sickle cell disease and others.
This research is the latest development in a decade-plus of focused research in adoptive immunotherapy within the Center for Cancer and Immunology Research and the Sheikh Zayed Institute for Pediatric Surgical Innovation.
What’s next
The authors write that there are several critical areas for future research to advance this approach, including a need to understand the specific T cell component and receptors involved in recognizing tumor antigens. They will also need to explore the longevity of the trained T cell response including studies of the memory and persistence of trained PBMCs to ensure lasting anti-tumor effects. Finally, the team will explore the risk of T cell exhaustion, which could reduce the effectiveness of the therapy over time.
Though work remains, the authors note, “Our findings lay the groundwork for developing this approach into a viable therapy for neuroblastoma and possibly other solid tumors as well.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/06/cancer-cells-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-06-09 10:03:082025-06-09 10:05:08Preliminary study points to efficacy of PBMC-based immunotherapy for neuroblastoma
A new HIV-specific T cell therapy, tested in six adults living with HIV, used specially trained immune cells made from each person’s own blood — a personalized therapy designed to target the virus with precision.
An exciting small clinical trial led by the Center for Cancer and Immunology Research at Children’s National Hospital has shown that a new HIV-specific T cell therapy is safe and may help reduce hidden reservoirs of the virus in the body. This approach, tested in six adults living with HIV, uses specially trained immune cells made from each person’s own blood — a personalized therapy designed to target the virus with precision.
The results, published in Nature Communications, represent a step forward in the search for a long-term, drug-free way to control or even cure HIV.
A smarter way to fight HIV
Today, people living with HIV rely on anti-retroviral therapy (ART) to keep the virus under control. These medications are highly effective but must be taken daily and do not eliminate the virus entirely. That is because HIV can hide in a “reservoir” of cells where it remains dormant and invisible to both drugs and the immune system. If ART is stopped, the virus can quickly return.
To change that, scientists at Children’s National and partnering institutions developed a new type of cellular therapy called HST-NEETs — short for “HIV-specific T cells targeting conserved epitopes”. These T cells are trained in the lab to recognize parts of the virus that do not change much, even as HIV mutates. This makes it harder for the virus to escape. The goal is to help the immune system find and destroy the infected cells that are normally hidden.
Safe and promising results
In this phase 1 clinical trial, researchers created personalized HST-NEET therapy from each participant’s own immune cells. After training the cells to recognize HIV, they were infused back into the patients twice over a period of weeks.
The results showed that:
No serious side effects were reported from the infusions.
The treatment was well-tolerated by all six participants.
In two people, the therapy led to stronger HIV-specific immune responses, including more virus-fighting T cells and antibodies.
In two others, researchers saw a drop in the level of HIV hidden in their cells, a sign that the virus reservoir might be shrinking.
In four participants, the infused T cells persisted in the bloodstream for up to 40 weeks, continuing to patrol for signs of HIV.
While not a cure, these findings show early evidence that the therapy may help the body better recognize and fight HIV, even the hidden forms that are hardest to treat.
Building toward a cure
“The fact that we saw HIV-specific T cell responses increase in some participants, even without additional immune-boosting drugs, is very encouraging,” said Catherine Bollard, MBChB, MD, senior author of the study and director of the Center for Cancer and Immunology Research at Children’s National. “It suggests that the immune system can be trained to go after parts of the virus that were previously out of reach.”
Unlike bone marrow transplants, which have led to a cure in a few people with both HIV and cancer but carry high risk, HST-NEET therapy is much safer and more scalable. That is important for the millions of people living with HIV worldwide.
This study also sets the stage for future clinical trials that could combine T cell therapy with other strategies, like latency-reversing drugs that “wake up” hidden HIV, to further shrink the reservoir. It also shows that personalized T cells can be safely made, infused and tracked over time and that they can continue working in the body for many months. Those lessons are valuable not just for HIV but also for developing safer, more targeted cancer immunotherapies in children and adults.
What’s next
The next phase of research will evaluate this therapy in larger groups and under different conditions, including in people undergoing stem cell transplants or with added immune system boosters. Clinical trials are already underway exploring these combinations.
By focusing on preserved parts of the virus, the regions that HIV cannot easily mutate, HST-NEETs could one day become part of a combination approach to eliminate HIV from the body altogether.
“Every step brings us closer to a functional cure,” said Dr. Bollard. “And the lessons we’re learning from HIV may also inform how we treat other chronic viral infections, and even cancer, in the future.”
Authors authors from Children’s National include Danielle K. Sohai, Michael D. Keller, Patrick J. Hanley, Fahmida Hoq, Divyesh Kukadiya, Anushree Datar, Emily Reynolds, Christopher Lazarski, Chase D. McCann, Jay Tanna, Abeer Shibli, Haili Lang, Anqing Zhang, Pamela A. Chansky, Cecilia Motta and Conrad Russell Y. Cruz.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/tube-rack-in-lab-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-05-23 12:34:312025-05-23 12:35:29Personalized T cell therapy for HIV shows safety and early signs of impact
Children’s National Hospital hosted its fifteenth annual Research, Education and Innovation Week from March 31–April 4, 2025, bringing together clinicians, scientists, educators and innovators from across the institution to celebrate discovery and collaboration. This year’s theme, “Empowering the Future in Pediatric Research and Innovation with Equity, Technology and a Global Reach,” served as a call to action for advancing science that improves child health both locally and around the world.
Each day of the week-long event featured thought-provoking lectures — now available to watch — dynamic panel discussions, interactive workshops and vibrant poster sessions, all highlighting the diverse and interdisciplinary work taking place across Children’s National.
Centering the patient and the planet
REI Week began on Monday with a powerful keynote lecture from Lynn R. Goldman, MD, MS, MPH, Michael and Lori Milken dean of the Milken Institute School of Public Health at the George Washington University. In her talk, “Children: Uniquely vulnerable to climate-related threats,” Dr. Goldman underscored the urgent need to protect children from the environmental hazards of a changing climate and to integrate climate science into pediatric care and advocacy.
At mid-morning, Mary-Anne “Annie” Hartley, MD, PhD, MPH, director of the LiGHT Laboratory at École Polytechnique Fédérale de Lausanne, introduced the “MOOVE” platform — Massive Open Online Validation and Evaluation of clinical LLMs. Her talk demonstrated how artificial intelligence, when rigorously validated, has the potential to transform clinical decision-making and global health equity.
Monday’s final keynote, “Zinc and childhood diarrhea,” was presented by Christopher Duggan, MD, MPH, director of the Division of Nutrition at Harvard Medical School. Dr. Duggan highlighted the global health impact of zinc supplementation in reducing childhood mortality — a reminder that simple, evidence-based interventions can save millions of lives.
In that first day, the first poster session of the week showcased projects in adolescent medicine, global health, infectious diseases, oncology and more. The session reflected the full breadth of research taking place across Children’s National.
Ambroise Wonkam, MD, PhD, professor of genetic medicine at Johns Hopkins University, then delivered Tuesday’s Global Health Keynote Lecture, “Harnessing our common African genomes to improve health and equity globally.” His work affirmed that inclusive genomics is key to building a healthier world.
Later, the Global Health Initiative event and GCAF Faculty Seminar encouraged attendees to pursue collaborative opportunities at home and abroad, reflecting the growing global footprint of Children’s National research programs.
Transforming education and care delivery
On Wednesday, Larrie Greenberg, MD, professor emeritus of pediatrics, kicked off the day with a Grand Rounds keynote on educational transformation: “Shouldn’t teachers be more collaborative with their learners?” He followed with a CAPE workshop exploring the effectiveness of case-based learning.
In the Jill Joseph Grand Rounds Lecture, Deena J. Chisolm, PhD, director of the Center for Child Health Equity at Nationwide Children’s Hospital, challenged attendees to move beyond dialogue into action in her talk, “Health equity: A scream to a whisper?,” reminding researchers and clinicians that advocacy and equity must be foundational to care.
The day continued with a poster session spotlighting medical education, neonatology, urology and neuroscience, among other fields.
Posters and pathways to progress
Throughout the week, poster sessions highlighted cutting-edge work across dozens of pediatric disciplines. These sessions gave attendees the opportunity to engage directly with investigators and reflect on the shared mission of discovery across multiple disciplines, including:
The REI Week 2025 Awards Ceremony celebrated outstanding contributions in research, mentorship, education and innovation. The winners in each category were:
POSTER SESSION AWARDS
Basic & Translational Research
Faculty: Benjamin Liu, PhD
“Genetic Conservation and Diversity of SARS-CoV-2 Envelope Gene Across Variants of Concern”
Faculty: Steve Hui, PhD
“Brain Metabolites in Neonates of Mothers with COVID-19 Infection During Pregnancy”
Faculty: Raj Shekhar, PhD
“StrepApp: Deep Learning-Based Identification of Group A Streptococcal (GAS) Pharyngitis”
Post docs/Fellows/Residents: Dae-young Kim, PhD
“mhGPT: A Lightweight Domain-Specific Language Model for Mental Health Analysis”
Post docs/Fellows/Residents: Leandros Boukas, MD, PhD
“De Novo Variant Identification From Duo Long-Read Sequencing: Improving Equitable Variant Interpretation for Diverse Family Structures”
Staff: Naseem Maghzian
“Adoptive T Lymphocyte Administration for Chronic Norovirus Treatment in Immunocompromised Hosts (ATLANTIC)”
Graduate Students: Abigail Haffey
“Synergistic Integration of TCR and CAR T Cell Platforms for Enhanced Adoptive Immunotherapy in Brain Tumors”
High School/Undergraduate Students: Medha Pappula
“An ADHD Diagnostic Interface Based on EEG Spectrograms and Deep Learning Techniques”
Clinical Research
Faculty: Folasade Ogunlesi, MD
“Poor Air Quality in Sub-Saharan Africa is Associated with Increase Health Care Utilization for Pain in Sickle Cell Disease Patients”
Faculty: Ayman Saleh, MD
“Growth Parameters and Treatment Approaches in Pediatric ADHD: Examining Differences Across Race”
Post docs/Fellows/Residents: Nicholas Dimenstein, MD, MPH
“Pre-Exposure Prophylaxis (PrEP) Eligibility in the Pediatric Emergency Department”
Staff: Tayla Smith, MPH
“The Public Health Impact of State-Level Abortion and Firearm Laws on Health Outcomes”
Graduate Students: Natalie Ewing
“Patterns of Bacteriuria and Antimicrobial Resistance in Patients Presenting for Primary Cloacal Repair: Is Assisted Bladder Emptying Associated with Bacteriuria?”
Graduate Students: Manuela Iglesias, MS
“Exploring the Relationship Between Child Opportunity Index and Bayley-III Scores in Young Children”
High School/Undergraduate Students: Nicholas Lohman
“Preliminary Findings: The Efficacy, Feasibility and Acceptability of Group Videoconference Cognitive Behavioral Therapy with Exposure and Response Prevention for Treating Obsessive-Compulsive Disorder Among Children and Young People”
Community-Based Research
Faculty: Sharon Shih, PhD “Assessing Pediatric Behavioral Health Access in DC using Secret Shopper Methodology”
Post docs/Fellows/Residents: Georgios Sanidas, MD “Arrested Neuronal Maturation and Development in the Cerebellum of Preterm Infants”
Staff: Sanam Parwani
“Intersectionality of Gender and Sexuality Diversity in Autistic and Non-Autistic Individuals”
Graduate Student: Margaret Dearey “Assessing the Burden of Period Poverty for Youth and Adolescents in Washington, DC: A Pilot Study”
Quality and Performance Improvement
Faculty: Nichole L. McCollum, MD
“A Quality Improvement Study to Increase Nurse Initiated Care from Triage and Improve Timeliness to Care”
Post docs/Fellows/Residents: Hannah Rodriguez, MD
“Reducing Unnecessary Antibiotic Use in a Level IV NICU”
Staff: Amber K. Shojaie, OTD, OTR/L
“Implementing Dynamic Axilla Splints in a Large Burn Patient”
Meleah Boyle, PhD, MPH
“Understanding and Addressing Environmental Sustainability to Protect the Health of the Children’s National and Global Communities”
Eiman Abdulrahman, MD
“Research Capacity Building to Improve Pediatric Emergency and Critical Care in Ethiopia”
Pilot Awards
Alexander Andrews, MD
“EEG as a Diagnostic and Prognostic Marker in Severe Pediatric Malaria, Blantyre Malawi”
Daniel Donoho, MD & Timothy Singer, MD
“Feasibility Study of a Novel Artificial Intelligence-Based Educational Platform to Improve Neurosurgical Operative Skills in Tanzania”
Hasan Syed, MD
“Bridging the Gap an Educational Needs Assessment for Pediatric Neurosurgery Training in Pakistan”
Sofia Perazzo, MD & Lamia Soghier, MD, MEd, MBA
“QI Mentorship to Improve Pediatric Screening and Follow-up in Rural Argentina”
Benjamin Liu, PhD
“AI-Empowered Real-Time Sequencing Assay for Rapid Detection of Schistosomiasis in Senegal”
Rae Mittal, MD
“Assessment and Enhancement of Proficiency in Emergency Child Neurology Topics for Post-Graduate Emergency Medicine Trainees in India”
Innovation Day ignites bold thinking
Thursday, REI Week shifted to the Children’s National Research & Innovation Campus for Innovation Day, a celebration of how bold ideas and collaborative culture can accelerate progress in pediatric medicine.
REI Week 2025 reaffirmed the values that define Children’s National: a commitment to excellence, collaboration and equity in pediatric research and care. As discoveries continue to emerge from our hospital and our research campuses, the connections built and ideas sparked during this week will help shape the future of pediatric health — locally and globally.
By elevating voices from the bedside to the bench, with the support of the executive sponsors Nathan Kuppermann, MD, MBChB, Catherine Bollard, MBChB, MD, Kerstin Hildebrandt, MSHS, Linda Talley, MS, RN, NE-BC and David Wessel, MD, REI Week demonstrated that we must embrace the community in all aspects of our work. Because we know that there are answers we can only get from the patients that we serve—and we need to be their voice.
Research, Education & Innovation Week will be back next year on April 13-17, 2026.
Posters at the REI Week 2025 Monday, March 31 poster session.
Panelists discuss innovation during REI Week 2025.
Global Health Initiative community engagement event during REI Week 2025.
Chris Rees presents his REI Week 2025 lecture.
Nathan Kuppermann listens to a presenter during the REI Week 2025 Tuesday, April 1, poster session.
Michelle Riley-Brown, Nathan Kuppermann, Catherine Bollard and Naomi Luban on stage during the REI Week 2025 awards ceremony.
Brandy Salmon presents on innovation programs at Virginia Tech during the REI Week 2025 Innovation Day.
Catherine Bollard listens to a presenter during the REI Week 2025 Monday, March 21 poster session.
Ambroise Wonkman poses for a picture with Children’s National staff.
Tanzeem Choudhury presenting during REI Week 2025.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/REI-Week-2025-Monday-Poster-Session-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-04-22 10:31:052025-06-10 12:20:52REI Week 2025 empowers the future in pediatric research and innovation
Jo Lynne Rokita, PhD, is the director of the new Bioinformatics Core housed within the Brain Tumor Institute at Children’s National Hospital.
Jo Lynne Rokita, PhD, is the director of the new Bioinformatics Core housed within the Brain Tumor Institute at Children’s National Hospital. Dr. Rokita is a cancer genomics leader with 20 years of combined research experience in academia, industry and the government. She’s also a technical and analytical expert in genomics research using microarrays and high-throughput sequencing.
“We are very excited that we were able to recruit Dr. Rokita as director of the Bioinformatics Core Facility,” says Muller Fabbri, MD, PhD, associate center director for Cancer and Immunology Research at Children’s National. “Her Bioinformatics Core will play a central role in providing the Brain Tumor Institute community with unique expertise spanning biology/genetics/genomics and bioinformatics and will propel Children’s National forward as a national and worldwide leader in pediatric brain tumor research.”
Dr. Rokita is overseeing the core’s creation, including bringing both bioinformatics staff and computing infrastructure to the program, which will support the data analysis needs of the institute’s investigators. She recently answered questions about the new core and also talked a little bit about the focus of her own research that will continue at Children’s National.
Q: Why is the Brain Tumor Institute establishing a Bioinformatics Core?
A: Growing the institute’s bioinformatics capabilities was one of the things that leadership wanted to make sure was built into the plan for the record-setting $96 million gift that was received in 2023. There was a clear need among the principal investigators for this type of research support which includes organization, analysis and interpretation of large-scale genetic sequencing and other “-omics” data.
Q: How did you decide to join Children’s National?
A: I was leading a pediatric brain tumor focused bioinformatics team at Children’s Hospital of Philadelphia (CHOP). As a part of the Children’s Brain Tumor Network (CBTN), I worked closely with a collaborator from Children’s National, Brian Rood, MD, medical director of the Brain Tumor Institute. He told me about the opportunity and I was very excited to apply.
Q: How did your previous work prepare you for this role?
A: I’ve spent the past 10 years in the pediatric cancer field with the last six focused on brain tumor research. In my various roles at CHOP, I led multiple large-scale genomic analysis efforts, comprehensive data and methods for which we then provided openly to the community. During my postdoctoral fellowship, these efforts included a large neuroblastoma patient-derived cell line “ENCODE” as well as a resource led in collaboration with multiple institutes and the National Cancer Institute funded by Alex’s Lemonade Stand Foundation (ALSF). We further scaled these efforts to build open analytical platforms to empower researchers to build upon our work doing their own cancer genomic analysis. In collaboration with the Childhood Cancer Data Lab at ALSF, we built the platform that ultimately ballooned into the OpenPedCan includes large amounts of harmonized genomic, epigenomic and proteomic data for patients with pediatric cancer. What’s unique is that the data is all processed in the same way and easily accessible through multiple mechanisms. Researchers can use these data to ask questions about the cancer type they study or genes of interest. For example, genes over-expressed, absent and/or mutated in a specific tumor subtype may lead to a better understanding of how a patient’s cancer may respond to a treatment.
We’ll be bringing some of the workflows we created previously here to Children’s National, and that will allow us to join newly generated internal data with the thousands of data points we’ve already harmonized using these workflows.
Q: Can you give us some examples of how data harmonization benefits the field of pediatric brain tumor research?
A: Harmonizing across institutions and databases will help us increase the number of data points available for study. This is really important for rare types of tumors and are major foci of institute collaborator Adriana Fonseca, MD, and her International Rare Brain Tumor Registry program. The Bioinformatics Core will support data organization and analysis for this effort, which aims to sequence the rarest brain tumors — those that make up between only 3% and 5% of all brain tumors. If all the data is analyzed the same way, we can combine multiple studies to increase our total dataset, which in turn may reveal new biomarkers and new subtypes of those tumors. It is critical that we continue to build these data resources in a way that they can be accessed by everyone doing this work. Having dedicated support systems for these functions will push the research farther, faster.
Q: As this work gets underway, what is the core’s main function?
A: As this initiative gets underway, the Bioinformatics Core’s primary goal is to empower investigators by streamlining and centralizing data analyses. We help researchers transfer sequencing data into secure cloud storage, organize newly generated records and prepare those datasets for in-depth study. Our bioinformatics scientists then perform downstream analyses to address the specific questions posed by each investigator. On the backend, we collaborate with information technology at Children’s National to develop a robust infrastructure that supports these activities efficiently. By offering these services in-house, we aim to ensure our investigators have seamless, comprehensive support—ultimately driving innovation and accelerating research progress.
Q: What is “open science” and why is it important in bioinformatics?
A: One of our big focus areas is open science, meaning our goal is to push data and code out into the community so that researchers can easily reproduce and build upon our findings. I’m excited to bring the principles of open science, code sharing and data sharing to the Bioinformatics Core.
Making resources open makes it easier for teams to work together across institutions and research programs. It is also going to benefit patients because people can reuse the code and move towards cures faster. For example, we try to package an entire manuscript’s code when we provide our data so it’s clear how the analyses were done.
Q: What is your particular research passion?
A: I work in several research areas and with many brilliant collaborators. One of our focus areas is understanding how RNA splicing can contribute to pediatric brain tumors to create a change in a protein. We have recently identified tumor-specific splice events in some pediatric brain tumor types and will be partnering with Dalia Haydar, PharmD, PhD, to create therapeutic approaches to targeting these. We are also developing a user-friendly application for mining the large amount of splicing data in pediatric brain tumors.
Another focus of our lab is understanding how the patient’s host genome (alterations inherent in their blood DNA) influences the tumor’s genetics. For example, we’ve just preprinted a study connecting inherited variants to tumor genetics and patient outcomes.
Finally, we are interested in how differences in race, ethnicity and social determinants of health influence survival and treatment outcomes for children with brain tumors.
I am passionate about data sharing, code reproducibility and promoting open science in general.
Q: Is there any specific reason you decided to focus your work around brain tumors and pediatric brain tumors?
A: My cousin passed away from a brain tumor when I was in high school. They didn’t have molecular diagnosis then, but he had a brainstem glioma, likely a diffuse midline glioma. In graduate school, I studied addiction genetics and became fascinated with the brain and towards the end, cancer. As an alumna of Penn State, I was actively involved in philanthropic events raising money for their Dance MaraTHON supporting children with cancer. I was lucky to land a postdoc at CHOP and lean into subsequent roles which allowed my passion for this field to grow.
Q: Last question — What do you do with your time when you are not studying pediatric brain tumor data?
A: I enjoy being with my family, observing my children learn and grow, and listening to music.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/bioinformatics-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-02-26 16:09:002025-03-06 13:18:03Q&A with Dr. Rokita: Building bioinformatics infrastructure at the Brain Tumor Institute
The new partnership will advance pediatric health through innovative discoveries and therapies, with an initial focus on pediatric cancers, including brain tumors.
Children’s National Hospital and Virginia Tech are expanding their research partnership, building on a successful collaboration established in 2019. This partnership will advance pediatric health through innovative discoveries and therapies, with an initial focus on pediatric cancers, including brain tumors.
The partnership brings together Children’s National, ranked among the nation’s top pediatric hospitals by U.S. News & World Report, and Virginia Tech, a leading academic research institution. Together, they aim to deliver transformative advancements to enhance outcomes for children facing devastating diagnoses.
The goals of the research-focused partnership include:
Accelerating the understanding of the biology, improvements in prevention and treatment of pediatric cancers and other childhood diseases.
Developing new diagnostic and therapeutic tools to improve care for children.
Training the next generation of scientists and physician-scientists.
What they’re saying
“Over the years, our partnership with Virginia Tech has demonstrated the power of combining top-tier research expertise with a shared commitment to improving pediatric health,” said Catherine Bollard, MBChB, MD, senior vice president and chief research officer and director of the Center for Cancer and Immunology Research. “This expansion underscores our belief that by working together, we can accelerate discoveries and develop life-changing therapies for children with cancer and other rare diseases.”
“Children’s National Hospital has been an important partner for us in biomedical research and innovation,” said Michael Friedlander, PhD, Virginia Tech vice president for health sciences and technology. “Our collaboration deepened with the launch of Children’s National Research & Innovation Campus in Washington, D.C., and now, as our partnership grows even stronger, we’re poised together to take on some of the biggest challenges in cancer research to contribute to the health of children and adults.”
“Partnering with Children’s National connects us to a world-class clinical trial institute that has been a pioneer in treating brain tumors with focused ultrasound technology, and this presents a unique opportunity to help children and families struggling with cancer,” said Cheng-Chia “Fred” Wu, MD, PhD, a member of the Children’s National Brain Tumor Research Institute and a principal investigator in cancer research and faculty member at the Fralin Biomedical Research Institute in Roanoke and in the Virginia Tech Carilion School of Medicine.“I can’t wait to see where this takes us.”
Big picture
The initial focus of the collaboration is pediatric cancers, including brain tumors — among the most challenging childhood diagnoses. By combining Virginia Tech’s leading-edge technology and research infrastructure with Children’s National’s expertise in pediatric care, the organizations aim to make significant strides in understanding these diseases.
An interdisciplinary approach is at the heart of the ongoing strategy. The collaboration first began with the launch of a 12,000-square-foot Virginia Tech biomedical research facility within the Children’s National Research & Innovation Campus, which opened in 2020. Located on a 12-acre portion of the former Walter Reed Army Medical Center in Washington, D.C., the campus was the nation’s first innovation hub focused exclusively on pediatric research.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/boy-getting-eye-exam-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-02-04 13:31:522025-02-04 13:32:49Expanded partnership with Virginia Tech accelerates pediatric cancer research
The Children’s National 2023-2024 Academic Annual Report show on a tablet.
Children’s National Hospital has released its 2023-2024 Academic Annual Report, showcasing a year of transformative progress in pediatric medicine. The report highlights achievements across its research centers, institutes and Innovation Ventures, underscoring the hospital’s role as a leader in advancing child health through innovation and collaboration.
“This year’s report reflects the remarkable progress we have made in advancing the frontiers of pediatric medicine,” said Nathan Kuppermann, MD, MPH, Chief Academic Officer and Chair of Pediatrics. “It highlights groundbreaking work across our research centers, institutes, and Innovation Ventures, showcasing the collaborative spirit that drives our mission forward. These achievements underscore our shared commitment to delivering transformative research and the best possible outcomes for children and families.”
Delivering across centers
The report captures the contributions of each of Children’s National’s research centers, each pushing the boundaries of pediatric healthcare:
Center for Cancer & Immunology Research (CCIR): Delivering on the promise of cell and gene therapies, offering innovative treatments for pediatric cancers and immune disorders.
Center for Genetic Medicine Research (CGMR): Advancing pediatric genetic medicine through interdisciplinary efforts, addressing complex genetic conditions with cutting-edge science.
Center for Neuroscience Research (CNR): A year of growth in scientific excellence, advancing the understanding of brain development and neurological conditions.
Center for Prenatal, Neonatal & Maternal Health Research (CPHNMR): Revolutionizing neonatal care with its pioneering infant brain health neuromonitoring program.
Center for Translational Research (CTR): Facilitating groundbreaking work by new K awardees and driving translational research to bridge the gap between discovery and clinical care.
Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI): Leading the way in advanced research projects in pediatric surgery, pushing technological boundaries to improve outcomes for children worldwide.
Taking the lead in innovation through collaboration
Innovation Ventures at Children’s National is advancing pediatric health security, addressing unique challenges with transformative solutions. Meanwhile, the Children’s National Research & Innovation Campus (CNRIC) continues to thrive as a hub for discovery and collaboration, hosting conferences on topics like artificial intelligence in healthcare, cell and gene therapy, and pediatric epilepsy research.
A vision for the future
The report also highlights Children’s National’s focus on integrating cutting-edge technologies like artificial intelligence into its research and clinical practices, as well as addressing global health challenges such as the effects of climate change on children’s health. These efforts reflect the hospital’s commitment to improving outcomes for children everywhere through innovation, teamwork, and forward-thinking leadership.
The 2023-2024 Academic Annual Report serves as a testament to the dedication and expertise of the Children’s National community, showcasing how collaboration and innovation are shaping the future of pediatric healthcare.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/01/2023-2024-Academic-Annual-Report-cover-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-01-13 13:51:482025-01-13 13:53:49Children’s National delivers on the promise in 2024
Nearly 200 biomedical leaders from Washington, D.C., Maryland, and Virginia gathered at the Children’s National Research & Innovation Campus for the 2nd annual Cell & Gene Therapy Symposium. The event showcased groundbreaking developments in rare disease treatments and underscored the importance of regional collaboration.
“By targeting diseases at the cellular level, we are on the cusp of breakthroughs in cell and gene therapy that will transform medicine,” said Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research (CCIR) at Children’s National Hospital and a host of the symposium. “Progress will accelerate if we build partnerships beyond our own organizations.”
The big picture
Scientists and clinicians have worked for more than two decades to develop cell and gene therapies aimed at treating diseases on a cellular level. The past few years have been particularly promising as investment in science has led to advancements. Children’s National is at the forefront, as one of the first pediatric hospitals in the world to offer commercial gene therapies for sickle cell disease.
Many more treatments for rare diseases are in development at Children’s National and beyond. Leaders at CCIR are actively building collaborations with companies, academic institutions and enterprises across the mid-Atlantic region to accelerate these efforts.
During the symposium, Eugene Hwang, M.D., chief of Oncology at Children’s National, addressed the urgent need for more effective and less toxic treatments for pediatric brain tumors. He highlighted the potential of combining immunotherapies with innovations like low-intensity focused ultrasound, which can open the blood-brain barrier temporarily to improve drug delivery to tumors.
“With collaboration between the lab and clinic, alongside industry partners and even between hospitals, we can finally make strides I haven’t seen in my entire career,” Dr. Hwang said. “It’s an incredibly inspiring time for all of us.”
Why it matters
Experts from organizations as diverse as MaxCyte, ScaleReady, RoosterBio, PSC Biotech, Qiagen, FujiFilm and the Frederick County Office of Economic Development came together for the daylong conversation.
Michael Friedlander, Ph.D., executive director of the Fralin Biomedical Research Institute at Virginia Tech, emphasized the critical role of regional partnerships in fulfilling the potential of these emerging therapies. He pointed to the collaborative research between Children’s National and Virginia Tech on brain tumors, where bioengineers and cancer researchers are working side-by-side to create new treatments.
“We are now able to begin delivering these leading-edge therapies to patients,” Dr. Friedlander said. “For example, those who live in rural settings often have much less access to such frontline medical innovations. By collaborating with Children’s National and gaining access to urban pediatric populations, as well as patients in our more rural area, we can start to bring these therapies to a much broader audience.”
What’s next
Patrick Hanley, Ph.D., chief and director of the Cellular Therapy Program at Children’s National, observed that other regions in the U.S. are uniting to advance scientific discoveries with the backing of government, academia and industry. He hopes to see similar collaboration across the D.C., Maryland, and Virginia area, known as the DMV. Children’s National is leading an initiative called CHARM – the Capital Health and Mid-Atlantic Regenerative Medicine – to bring regional experts together for webinars, networking events and partnership opportunities.
“There’s significant interest in cell and gene therapy worldwide,” said Dr. Hanley, a symposium host. “I see an even greater interest in creating cell and gene therapy hubs. The time is right for our mid-Atlantic region, and I’m excited to see what unfolds in the next five years.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/11/CGT-Conference-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-11-26 10:13:282024-11-26 10:15:14Regional powerhouse: Cell and Gene therapy leaders from mid-Atlantic forge connections
On November 1, Children’s National Hospital installed AeRang Kim, M.D., Ph.D., as the first holder of The Lexi Speight Chair in Pediatric Oncology.
Dr. Kim is clinical research director for the Oncology Division within the Cancer and Blood Disorders Center at Children’s National. She is a tenured professor of pediatrics at the George Washington University School of Medicine and Health Sciences.
The big picture
Dr. Kim joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair. Children’s National is grateful to generous donors who altogether have funded 49 professorships.
Professorships support groundbreaking work on behalf of children and their families and foster new discoveries and innovations in pediatric medicine. These appointments carry prestige and honor that reflect the recipient’s achievements and donor’s commitment to advancing and sustaining knowledge.
Why it matters
Since arriving at Children’s National in 2010, Dr. Kim has played a pivotal role in our solid tumor program. She leads the renowned multi-disciplinary Sarcoma Clinic, which includes a comprehensive team of oncologists, nurses, orthopedic surgeons, radiologists, a genetic counselor and a physical therapist. It is one of the few of its kind in the country. Dr. Kim’s dedication and leadership have been instrumental in earning Children’s National recognition as a Sarcoma Alliance Center of Excellence.
Dr. Kim leads clinical trials evaluating new pediatric solid tumor treatments across multiple institutions. She pioneers precision approaches using targeted drugs, advanced devices and cell therapies. Her innovative work attracts numerous grants, including a recent $1.3 million from the Department of Defense.
“The future of cancer treatment is in precision medicine,” says Dr. Kim. “As The Lexi Speight Chair of Pediatric Oncology, I will explore new ways to design clinical trials to accelerate development of new therapies for solid tumors. This could change the paradigm for pediatric cancer treatment.”
Moving the field forward
The Speight family, through their vision and generosity, are ensuring that Dr. Kim and future holders of this chair will launch bold, new initiatives to rapidly advance the field of pediatric oncology, elevate our leadership and improve the lifetimes of children with solid tumors.
“When Lexi died, we had a decision to make about how to channel our grief,” Cyndi Speight, Lexi’s mom, remembered. “And do what we could to help other children and families from experiencing what we did.” And so, Cyndi, her husband Petr, and their daughter Sam established The Lexi Speight Chair in Pediatric Oncology with support from community partners in loving memory of Lexi. The Speight family started Laps for Lexi, an annual 5K run/walk that raised money for both pediatric cancer at Children’s National and a scholarship at Sandy Spring Friends School. This successful event ran for 13 years, bringing hope to children and families. The Speight family’s dedication and passion for advancing solid tumor care ensures that Lexi’s legacy lives on in our pursuit of better treatments for children.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/11/cnmc-speight-chair-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-11-04 11:39:522024-11-04 11:41:06Honor bestowed on AeRang Kim, M.D., Ph.D.
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2024-25 Best Children’s Hospitals annual rankings. This marks the eighth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
This year, U.S. News ended ordinal rankings on its Honor Roll. Instead of assigning a numerical rank from 1 to 10, all hospitals on the Honor Roll will be recognized as having attained the highest standards of care in the nation.
In addition, Children’s National tied for #1 pediatric hospital in the Mid-Atlantic region, which includes New York, New Jersey, Delaware, Pennsylvania, the District of Columbia, West Virginia and Virginia. It’s also best in the Mid-Atlantic in Neonatology.
For the fourteenth straight year, Children’s National ranked in 10 specialty services. New this year, U.S. News included behavioral health as a service line in the rankings. Since it’s the first year, there are no ordinal rankings for behavioral health, but the Children’s National program was named one of the top 50 programs in the country.
“In my first year here, I witnessed what makes Children’s National so special — our commitment to collaboration, empowering one another, and charting a bold path forward for pediatric care,” said Michelle Riley-Brown, MHA, FACHE, president and chief executive officer of Children’s National. “I’m proud U.S. News again recognized Children’s National as one of the top in the nation and the highest-ranked pediatric hospital in D.C., Maryland and Virginia. Together, we’ll continue to push the boundaries of care, research and innovation to make a difference for those who matter most — the kids.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“For nearly two decades, U.S. News has published Best Children’s Hospitals to empower the parents and caregivers of children with complex medical needs,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Children’s hospitals appearing on the U.S. News Honor Roll have a track record of delivering unparalleled specialized care.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/10/US-News-Badges-2024-25-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-10-08 01:00:002024-10-08 15:01:23Children’s National again ranked among the best in the nation by U.S. News & World Report
When new patients with chronic illnesses come to Roberta DeBiasi, M.D., M.S., division chief of Infectious Diseases, they are often drained of energy, far behind in school and fatigued by the lack of coordinated care among multiple specialists. She envisions a better way to care for these children: a data-driven, multidisciplinary clinic that can help diagnose and treat disorders facing chronically ill children.
In a keynote address, Dr. DeBiasi laid out her vision for improving care during the 7th annual symposium hosted by Children’s National Hospital and the National Institute of Allergy and Infectious Diseases (NIAID): “A new paradigm: Infection-associated chronic illnesses (IACI) affecting children.” Experts from across the country came together to discuss these IACIs, the importance of finding biomarkers to diagnose and monitor them, data-driven therapeutics to treat them, and the urgent need for protocols to guide physicians.
The patient benefit
A range of IACIs – including long COVID, Lyme disease, postural orthostatic tachycardia syndrome (POTS), dysautonomia and more – are stealing normal, active lifestyles from children. Dr. DeBiasi said patients need researchers who understand disease pathogenesis and have standardized disease classification to diagnose and treat these disorders. Because of the complexity of these cases, care delivery and coordination also need to change. Patients, she said, would best be served by beginning with a three-hour appointment in a multidisciplinary clinic with experts from behavioral health, rehabilitative medicine and other specialties.
“When one of these patients comes to us, we feel helpless as physicians,” Dr. DeBiasi said. “There’s no diagnostic, and we don’t know how to treat them…. It is, to me, very energizing that we’re going to be able to have a coordinated way to help these families. But to do that, we have to have standardized disease classification.”
Moving the field forward
In 2017, NIAID and Children’s National launched a clinical research partnership devoted to advancing the health of children with allergic, immunologic, auto-inflammatory and infectious diseases through collaborative research and education. The partnership — co-led by H. Clifford Lane, M.D., NIAID’s deputy director for Clinical Research and Special Projects, and Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research at Children’s National — promotes the prevention, diagnosis, treatment and cure of these childhood diseases. Every year, the partnership organizes and funds a symposium to explore cutting-edge research and pressing issues in pediatric care.
“There have been virtually no randomized, controlled trials and very little evidence on any sort of aggressive treatments, or pharmaceutical management options, especially in the pediatric population,” Dr. Yonts said. “Upon recent attendance at some long COVID meetings, there is an expressed concern, especially among pediatric providers, about trying medications off-label in these long COVID patients.”
Miss the symposium? You can learn more about the science they explored in the symposium’s recording on topics including:
Potential overarching mechanisms of disease, including pathogen- and host-mediated factors.
Identifying potential biomarkers for chronic illnesses
Treatments and multidisciplinary approaches for patients with IACIs
Patient advocacy
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/09/NIAID-Conference-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-09-23 15:18:322024-10-02 09:58:53Breaking free of illness: Experts explore solutions for chronic pediatric disorders
As researchers develop groundbreaking cellular therapies to treat pediatric solid tumors, physicians are preparing new ways to explain how these treatments work to patients and caregivers.
In a series of educational videos, scientists from Children’s National Hospital and institutions worldwide are offering tutorials on these novel treatments and how they target solid tumors at the cellular level.
“Let’s start by breaking down what a tumor-associated antigen-specific T (TAA-T) cell is,” Children’s National Research Technician Sammy Murphy says in one new video. “Our aim is to harness the power of T cells to identify and attack cancer cells.”
In less than six minutes, Murphy provides a short course on the details of these TAA-T cells and how her team combines their expertise in biology, medicine, bioinformatics, quality assurance and more to create the new therapies. “This collaborative team spirit has been a huge motivating factor and represents the best of what science can be,” she explains.
The big picture
Children’s National summer student Diana Kentell, a senior at Pratt Institute of Art studying digital art and 2D animation, created this video and a collection of others for the Cancer Grand Challenges (CGC), sponsored by the National Cancer Institute and Cancer Research UK. In 2022, the CGC awarded $25 million to Children’s National, the University College of London Cancer Institute and its partners on the NexTGen team to develop new therapies for pediatric solid tumors using CAR T cells.
The NexTGen team includes six patient advocates who have all been touched by pediatric tumors and support the scientists by providing the patient perspective on research and new treatments. These videos are a slice of the group’s efforts.
C. Russell Y. Cruz, M.D., Ph.D., a translational immunologist on the NexTGen team who oversaw Kentell’s video project, says bridging the gap between scientists and their patients who enroll in clinical trials will be essential to ensuring patients weigh the possibilities and the risks.
“Patient advocates help us understand our work from their perspective, making our science accessible to everyone,” Dr. Cruz said. “Engaging with such dedicated individuals often helps us refine our own ideas and provides invaluable insights. Most importantly, they remind us of our ultimate goal: to free future generations from the burden of pediatric cancer.”
Why we’re excited
In addition to the video on TAA-T cells, the team has assembled a collection of videos on killing assays, tumor slice assays and CAR T-cell manufacturing, which will help patients learn about the treatments when the clinical trials start. Sara Wakeling, who leads the NexTGen team’s patient advocates, said this toolkit will be a vital resource.
“Each of us came to this advocacy work because we were deeply affected by pediatric cancer. We aim to ensure that the child’s voice is central to the research and that the science is communicated in an informative and digestible way for patients’ families and the public,” Wakeling said. “With these videos, lay summaries of manuscripts and other explainers, we will have concrete information to share with families as soon as the new CAR T-cell therapies are ready for clinical trials.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/09/Cruz-video-still-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-09-13 11:35:042024-09-13 11:36:45What’s a TAA-T? Advocates create videos to translate science for patients
With CellBuilder and our global partnerships, Children’s National hopes to expand access to groundbreaking cell and gene therapy treatments as they take off in the next five years.
With cell and gene therapies poised to reshape cancer and rare disease treatments, researchers at Children’s National Hospital are pioneering ready-to-use solutions that will bring these cutting-edge therapies directly to hospitals and other treatment centers, shrinking the distance between doctors and patients.
“The next five years are going to be a period of tremendous growth for cell and gene therapy,” said Patrick Hanley, Ph.D., chief and director of the Cellular Therapy Program at Children’s National. “Currently, there’s no shortage of interest from the medical community, but there’s a shortage of people who can manufacture and administer this care. We’re looking for ways to get these treatments to the patients by providing other institutions the tools they need to launch these programs cost-effectively, safely and efficiently.”
Called CellBuilder, the starter kits for cell and gene therapy programs could transform the landscape for pediatric patients.
The big picture
Dr. Hanley and many members of the Children’s National team have been working in cell and gene therapy for more than a decade, gaining extensive experience in the technical and regulatory hurdles inherent in creating treatments that target diseases at their source.
In cell therapy, a specific cell type is modified and transferred to a patient with a payload that can target a disease or disorder. For example, T cells may be modified and delivered to patients to teach their immune systems to fight cancer. In gene therapy, a patient’s genetic code is modified to treat or prevent diseases, such as sickle cell disease, cancers and other genetic disorders. This can be done by introducing a healthy copy of a gene, repairing a faulty gene or altering a gene’s function.
Children’s National has become a leader in manufacturing virus-specific T cells, one method of delivering cell therapies, and the Cellular Therapy Program has conducted consortium-led, multi-center trials. Many other healthcare sites across the country want to start programs offering this care at their facilities.
The holdup in the field
Starting a cell and gene therapy program from scratch can take years of effort, training and money. That’s why Jay Tanna, M.S., R.A.C., quality assurance manager of the Cellular Therapy Program at Children’s National, said the team is creating CellBuilder starter kits, which include the manufacturing protocol and the resources necessary to launch a cell therapy program almost instantly.
“With a suitable knowledge base, institutions can start their own cellular therapy program at the point of care, using our manufacturing protocols, vetted reagents and other key elements of the process,” Tanna said. “Of course, interested institutions would have to meet regulatory requirements and establish a clean room to manufacture these therapies. If they want to use CellBuilder to run a clinical trial, they can do that. If they want to take it to become a licensed product, they can do that, too.”
Children’s National has worked with more than five institutions to build their virus-specific T-cell program and is now using the kits to accelerate and commercialize the process to increase patient access. The lab has also entered into a memorandum of understanding with the Tokyo-based Hitachi Global Life Solutions, Inc., an innovative modular clean room manufacturer, with the goal of offering a bundled solution.
Why we’re excited
Dr. Hanley and his colleagues say that the partnerships Children’s National is forging as they consult with other experts in this field will expand access to cell and gene therapy across the country—and hopefully around the world.
“It used to be that, to get a CAR T cell, you would collect the cells at Children’s National, ship them to a company like Novartis, have the therapy manufactured there and then shipped back,” said Michael Keller, M.D., who co-led a first-of-its kind immunotherapy trial as the Translational Research Laboratory director at the Children’s National Cell Enhancement and Technologies for Immunotherapy Program. “It was expensive, time-consuming and limited patient access. Now, there’s growing interest in manufacturing at each site, just like you would with a bone marrow transplant.”
With CellBuilder and our global partnerships, Children’s National hopes to expand access to groundbreaking cell and gene therapy treatments as they take off in the next five years, extending lifetimes and improving the quality of life for children suffering from rare disorders.
“We’re trying to capture the momentum underway in the field by providing this kit so that institutions don’t have to know how to do everything,” Dr. Hanley said. “We provide all the knowledge, a reagent list and everything else they need—and they provide the care.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/09/Clean-room-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-09-11 09:54:222024-10-02 09:55:58CellBuilder: A ready-made solution for cell & gene therapy manufacturing
Nathan Kuppermann, M.D., M.P.H., is taking on a pivotal role at Children’s National Hospital as executive vice president, the new chief academic officer (CAO) and chair of Pediatrics to continue growing the institution’s reputation as a world-class research hospital. He brings more than 30 years of clinical experience in pediatric emergency medicine and research to the leadership role, where he will oversee nearly 2,000 active research projects at the Children’s National Research Institute.
Dr. Kuppermann knows that science drives cures and improved outcomes. Early in his career, he received enhanced research training at the Harvard School of Public Health, where he laid the groundwork to become a globally recognized clinical researcher. He has studied when to order CT scans for children with head, abdominal and neck trauma to minimize radiation exposure, how to best manage children with diabetic ketoacidosis, infants with febrile illnesses and other complex questions in pediatric emergency medicine that require a multidisciplinary research approach to improve clinical care.
Dr. Kupperman is thrilled to join the scientific community in the nation’s capital, which he sees as a global city where he can authentically share his culturally rich background. He is the son of Brazilian immigrants — a chemical physicist and an organic chemist — and he married a pediatric endocrinologist whose parents are from Mexico and Germany. They have three daughters, and their youngest was adopted from Guatemala. As a family, they travel extensively, and he cares deeply about global health, having served as associate dean for Global Health at UC Davis.
A high school point guard who still plays basketball, Dr. Kuppermann runs his team’s offense on the court, choreographing the flow of each game to optimize his team’s strengths. The position requires peripheral vision to get the ball to the right player and make everyone look good. He sees parallels with his new role as CAO.
Q: What is your approach to research in pediatric healthcare?
A: Fundamentally, my philosophy around research is that we all need to collaborate. When I started doing my own research, I realized over time that to have big, impactful studies, two things had to happen: First, you need to work with people who have expertise beyond your own. I’m a big believer in team science and bench-to-bedside research, collaborating with people with complementary research skills.
Second, I realized that in pediatric research, you must collaborate in research networks to ensure your sample size has enough patients and patients from diverse populations to have definitive results and generalizable data.
Q: What values will you bring to the new role?
A: Three key elements come to mind. First, I’m a big believer in transparent communication, which is the root of everything good in life, whether it’s with your science, your friendships or your family.
I’m a big believer in team science. We all have certain areas of expertise, but if we want to combine our expertise to impact children and improve their health, we need to work together in teams, bringing together basic science researchers, clinicians, information technology specialists, knowledge-translation specialists and disseminators.
Finally, I am a cheerleader for science. As you develop your own science, you also are responsible for leading the next generation of scientists. I’ve spent as much time being a scientific mentor as I have working to discover new knowledge through scientific inquiry.
Q: You talk extensively about your family’s international roots and how it drives your work. What is the role of diversity in medicine and how does that guide you?
A: Diversity is fundamental to healthcare. We in the medical community recognize the disparities in the care we deliver, which I’ve studied in my research. Diversity must not only be a research focus, but our teams must be diverse to better investigate — and work to resolve — these inequities of care.
Children’s National is both a hospital that is mindful of its immediate community and an institution that greatly values the diversity of its patients and its staff. It’s also highly ranked in research and cares deeply about global health, all of which are drivers in my work.
When I considered the potential of coming to Children’s National, I thought I might be able to help this already great institution further its mission by serving its immediate community, growing and developing its global health programs, and taking research here from its already great bones and accomplishments to the next level.
Q: What approach do you bring to clinical care?
A: When I do a research study and enroll patients into a clinical trial, I think about the patient and others the research can impact. I frequently think of a quote by the late Paul Brodeur, a scientific writer who wrote a lot about asbestos, which is very powerful and meaningful to me: “Statistics are humans with the tears wiped away.”
And what it means to me is that we must be mindful as researchers that we’re talking about humans with our research. We’re not just talking about numbers, and we’re not just talking about getting grants and papers. We’re talking about how we can elevate the evidence and translate it to the bedside to improve the lives of humans.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/08/Kuppermann-video-still-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-09-03 12:32:372024-09-03 12:33:46Q&A with Dr. Kuppermann: Collaboration is critical for scientific success
Science is pioneering cures for pediatric rare diseases in a coming wave of new cell and gene therapies. However, the biopharmaceutical industry’s insistence on large patient populations and high profit margins may prevent these life-saving treatments from reaching the children who desperately need them. When successful therapeutics fail to see commercialization, experts say they have fallen into the “Valley of Death.”
To address this, leaders from pediatric healthcare, federal organizations, academia, industry and patient advocacy groups gathered at the Children’s National Research & Innovation Campus. Their objective: build a new framework to deliver these transformative drugs to clinics worldwide.
Meet the team forming Access4Kids, a nonprofit whose mission is to build new pathways to pay for cures and provide hope to children with life-limiting diseases. This group is working to change medicine and how we pay for it, under the leadership of Catherine Bollard, M.D., M.B.Ch.B., director of the Children’s National Center for Cancer and Immunology Research, Crystal Mackall, M.D., director of the Stanford Center for Cancer Cell Therapy, Julie Park, M.D., Oncology Department chair at St. Jude Children’s Research Hospital, and Alan Wayne, M.D., pediatrician-in-chief at Children’s Hospital Los Angeles.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/08/Manufacturing-Panel-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-08-22 15:48:542024-08-22 16:58:05Access4Kids: A new model to pay for pediatric cell and gene therapies
Cheng-Chia “Fred” Wu, M.D., Ph.D., joins the team at the campus as an assistant professor at Virginia Tech’s Fralin Biomedical Research Institute. Image credit: Fralin Biomedical Research Institute.
Experience, talent and technology are coming together at the Children’s National Research & Innovation Campus to solve the complex challenges of treating pediatric brain tumors through a growing partnership between Children’s National Hospital and Virginia Tech.
Cheng-Chia “Fred” Wu, M.D., Ph.D., joins the team at the campus as an assistant professor at Virginia Tech’s Fralin Biomedical Research Institute. He hopes to improve treatment for pediatric brain tumors and other cancers by leveraging technological advances in focused ultrasound and studying how this modality can be combined with other novel therapies. Children’s National physicians and scientists are collaborating with Virginia Tech scientists to develop these new approaches.
Why we’re excited
Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research and interim chief academic officer at Children’s National, said collaborations — including the partnership between Children’s National and Virginia Tech — are essential to solving formidable scientific challenges.
“We are thrilled to be working with Dr. Wu to develop cutting-edge therapeutics for pediatric brain tumors,” Dr. Bollard said. “With Dr. Wu’s experience and the talents of our team at Children’s National, I have great hope that we will be able to combine our novel technologies and therapies to provide tremendous breakthroughs for treating pediatric patients with brain tumors.”
Before joining Virginia Tech, Dr. Wu was an assistant professor of radiation oncology at Columbia University Irving Medical Center in New York, where he treated pediatric cancers and central nervous system malignancies.
“Partnering with Children’s National connects us to a world-class clinical trial institute that has been a pioneer in treating brain tumors with focused ultrasound technology, and this presents a unique opportunity to help children and families struggling with cancer,” Dr. Wu said. “I can’t wait to see where this takes us.”
Dr. Wu played a key role in the Initiative for Drug Delivery Innovation for Childhood Brain Tumors at Columbia, developing a bench-to-bedside platform to facilitate the translation of promising technologies for targeted drug delivery in children with brain tumors.
Within three years, the team demonstrated the safety and feasibility of using focused ultrasound in the brainstem and adding radiation in preclinical models. They then opened two clinical trials for kids with relapsed diffuse midline glioma, an aggressive and difficult-to-treat brain tumor that occurs in the brain stem, thalamus and spinal cord.
What’s ahead
Dr. Wu will be involved in a wide range of research touching both organizations, including veterinary medicine and biomedical engineering at Virginia Tech.
Michael Friedlander, Ph.D., executive director of the Fralin Biomedical Research Institute at Virginia Tech Carilion and vice president for health sciences and technology at Virginia Tech, welcomed Dr. Wu’s experience as a pediatric radiation oncologist, translational physician-scientist and clinical trialist who has led an innovative drug delivery program.
“He is armed with a unique set of skills to identify promising new technology and implement it in areas of great need for treatment of pediatric cancers,” Dr. Friedlander said. “We are absolutely delighted to have Dr. Wu as part of the team. He represents a powerful new part of the strong partnership between Virginia Tech and Children’s National Hospital for addressing pediatric brain cancer.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/08/Doctor-Wu-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-08-22 12:03:472024-08-22 12:04:52Expanding team innovates to take on pediatric brain tumors
Understanding and treating long COVID is still in its early days, but Dr. Yonts is beginning to see trends, along with hope for symptom relief.
A child who forgets the alphabet or spends 20 hours a day on the sofa will get a pediatrician’s attention. In late 2020, a stream of post-COVID patients just like this started presenting in the clinic of Alexandra Yonts, M.D., an infectious diseases specialist at Children’s National Hospital. Dr. Yonts quickly recognized the need to understand these patients and worked with hospital leadership to open the Pediatric Post-COVID Program, putting her at the forefront of clinicians and researchers investigating the disorder.
Understanding and treating long COVID is still in its early days, but Dr. Yonts is beginning to see trends, along with hope for symptom relief. She will present detailed data from a retrospective study of 254 post-COVID patients at the 2024 Children’s National-NIAID annual symposium, A New Paradigm: Infection-Associated Chronic Illnesses Affecting Children. She’ll discuss her findings on the patients’ symptoms at presentation, trajectory over time and a cluster analysis of symptom grouping. She gave an overview of her research and clinical work to Innovation District.
Q: What are you seeing in the Pediatric Post-COVID Program?
A: In the Infectious Diseases clinic, we had historically seen about one patient a month with prolonged fatigue or other persistent symptoms after an infection. Yet when COVID started, we noticed an increase in those patients. By late 2020, the numbers were increasing significantly, along with an uptick in appointment requests. We knew we needed to start a Pediatric Post-COVID Program, which launched in May 2021.
From the beginning and continuing to this day, severe fatigue is the most common reason kids come to our clinic, as is the case with adults. This ranges from marathon runners who can’t run a half-mile to those sleeping on the couch for 20 hours a day. We’re still researching the factors affecting this wide spectrum of symptoms.
Cognitive issues — often referred to as brain fog — are also significant. These can be seen as attention issues, such as difficulty remembering the alphabet in younger children or focusing in class for older children. Many kids have gastrointestinal problems like nausea, vomiting and abdominal pain. There’s also a prevalence of dysautonomia, affecting functions like blood pressure and heart rate, often seen in conditions like POTS (postural orthostatic tachycardia syndrome).
Initially, we saw kids infected early in the pandemic who had symptoms for 15 to 20 months. Our peak referrals were in 2022 after the Omicron variant, when we had a six-month waitlist. Although COVID cases have decreased, we still see kids with long-standing symptoms who have seen multiple providers without success. That’s why we’re here.
Q: Where are we in our understanding of long COVID, and where do we need to go?
A: We have lots of data but don’t know how it fits together yet. Research shows ongoing immune reactions to viral particles, with some patients having spike antigen in their blood or stool long after infection. There’s also evidence of autoimmunity and endovascular dysfunction, but we don’t yet understand the connections. It seems like viral persistence might be the underlying problem, but we haven’t pinpointed it yet.
Q: How important is it for the community to come together for events like the Children’s National-NIAID symposium?
A: It’s absolutely critical. We need researchers, clinicians and patients to collaborate. Researchers bring scientific expertise, clinicians provide practical insights and patients share their lived experiences and priorities. Conversations like the Children’s National-NIAID symposium are crucial for collaboration, thoughtful study design, advocacy and building connections with the patient community to make them feel validated and heard.
Learn more at the Children’s National-NIAID symposium on Sept. 5, by registering here.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/07/coronavirus-and-DNA-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-07-30 13:50:262024-07-30 13:55:20Untangling the root of long COVID with research
“To cure brain tumors, sickle cell disease and scores of other illnesses that have an outsized impact on pediatric patients, we will need an innovative mechanism to ensure that money is not a barrier to scientific advancement and world-class care,” says Dr. Bollard.
With the advent of life-changing cell and gene therapies (CGTs) to treat pediatric diseases, price is becoming a significant obstacle to care and cures.
Successful therapies can wind up shelved or in hard-to-reach clinical trials for a litany of reasons: high manufacturing costs, significant regulatory burdens, a lack of enthusiasm from the pharmaceutical industry in the small pediatric market and the simple fact that insurance companies resist paying the price of $1 million or more for a therapeutic. When successful treatments are set aside and become victims of this market failure, leaders in pediatric medicine say the drug has been relegated to the “Valley of Death.”
Experts at Children’s National Hospital and other leading U.S. research institutions are working to ferry drugs across it.
A new way forward
The Access4Kids think tank is bringing together healthcare leaders to chart another way – with its hosts Catherine Bollard, M.D., M.B.Ch.B., director of the Children’s National Center for Cancer and Immunology Research, Crystal Mackall, M.D., director of the Stanford Center for Cancer Cell Therapy, Julie Park, M.D., Oncology Department chair at St. Jude Children’s Research Hospital, and Alan Wayne, M.D., pediatrician-in-chief at Children’s Hospital Los Angeles. Organized at the Children’s National Research & Innovation Campus, the think tank will include voices from Seattle Children’s Hospital in Washington state and the Moonshot Presidential Office in Washington, D.C., along with experts from academic institutions, the federal government and patient advocacy groups.
They explained their vision in their recent Nature Medicine perspective, “Enhancing pediatric access to cell and gene therapies.” One idea under consideration is to create a biotech enterprise – backed by public monies, foundations and philanthropies – to support the late-stage development and commercialization of pediatric CGTs. Called a Pediatric Advanced Medicines Biotech (PAMB), this new organization would follow a novel pathway outside the traditional biopharma development model.
“To cure brain tumors, sickle cell disease and scores of other illnesses that have an outsized impact on pediatric patients, we will need an innovative mechanism to ensure that money is not a barrier to scientific advancement and world-class care,” Dr. Bollard said. “My colleagues and I aren’t exaggerating when we say this is a ‘save the world’ effort. It’s an initiative to disrupt the pharmaceutical industry and impact medicine, ultimately saving lives and entire lifetimes.”
The think tank is the second in a series aimed at solving this formidable challenge. Led by scientists, the work goes to the heart of healthcare economics.
“We need to find a way to support the academic ecosystem by reducing costs, creating efficiencies in manufacturing and working with regulatory bodies to bolster business models that lead to safe and effective therapeutics,” Dr. Mackall said. “We went to school to study science and medicine. Now, our mission includes revamping business models, as we find ways to increase access to lifesaving treatments for children in need.”
Why it matters
Creating novel pathways to pay for CGTs presents a challenge and an opportunity for researchers in pediatrics and rare diseases. Drs. Mackall, Bollard and their colleagues are exasperated when scientists discover successful treatments for life-threatening illnesses, but market forces lock the drug away in hard-to-reach clinical trials or – even worse – land it on a shelf.
Consider just one example, laid out in the Nature Medicine perspective: Children with adenosine deaminase-deficient severe combined immunodeficiency (ADA-SCID) lack nearly all protection from viruses, bacteria and fungi, leaving them vulnerable to a world of opportunistic organisms. Researchers at San Raffaele Telethon Institute for Gene Therapy in Italy won U.S. and European regulatory approvals for a gene replacement therapy to treat the life-threatening disorder. Yet currently the therapy is only available in clinical trials, with support from research grants, philanthropic donations and institutional resources.
“This happens to successful therapeutics, and it’s heartbreaking. The current business model in medicine can lead to situations where successful therapies have extremely restricted availability, and there are no built-in guarantees of sustained access,” Dr. Bollard said. “We can and must do better – and we believe we have a way forward.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/07/Bollard-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-07-19 08:00:292024-07-18 14:45:20Closing the ‘Valley of Death’: Pioneering – and paying for – new therapies
A Children’s National Hospital researcher is embarking on a two-year project that could revolutionize the care of rare pediatric brain tumors, through a Department of Defense (DOD) award to study the efficacy of combining the powers of acoustic therapy and cellular immunotherapy to treat the deadliest forms of medulloblastoma.
Designed by DOD to advance novel innovations that could revolutionize medicine, the prestigious Idea Award supports independent investigators with high-risk, but potentially high-reward, concepts to fill gaps in cancer prevention and treatment. Dalia Haydar, Pharm.D., Ph.D., principal investigator at the Cell Enhancement and Technologies for Immunotherapy Program, believes her first-of-its-kind approach could do just that.
A one-two punch
Dr. Haydar is building on promising research into a novel type of immunotherapy – chimeric antigen receptor (CAR) T-cell therapy – which uses the body’s own immune system to target and destroy pediatric brain tumors. She hopes to combine the potential of this immunotherapy with the early success seen in an acoustic therapy, called low-intensity focused ultrasound (LIFU). Akin to the imaging technology used during pregnancy, the sound waves can be directed toward any organ of the body for therapeutic reasons. With LIFU, Dr. Haydar hopes to tune the right amount of energy toward a brain tumor to temporarily open the blood-brain barrier and improve the delivery of therapeutics.
“We’re using two treatments that are tested in the clinic. We know how they work individually, but we’re investigating methods to combine the best aspects of both,” Dr. Haydar said. “I hope to use it, not just to open the channels in the blood-brain barrier, but also to cause a certain kind of immune response in the brain, which will help the CAR T-cells fight cancer.”
This collaborative grant includes experts in the field, including Yanxin Pei, Ph.D., principal investigator at Children’s National and an expert in medulloblastoma modeling, and Natasha Sheybani, Ph.D., assistant professor at the University of Virginia and a leading figure in the application of focused ultrasound.
Why we’re excited
Dr. Haydar is initially focused on high-risk medulloblastoma, specifically sonic hedgehog and group 3 subtypes, both of which are often fatal with existing chemotherapy and radiation treatments. Even when successful, the standard treatments can lead to life-long developmental side effects. Dr. Haydar hopes to show that the combined treatment improves survivorship, and she anticipates expanding her work to other types of pediatric brain tumors.
The $600,000 award shows the importance of well-resourced research institutions uniquely focused on pediatrics. Dr. Haydar noted that Children’s National is one of few research hospitals in the country with the necessary laboratory and ultrasound equipment on-site to develop a customizable treatment protocol. “We’re not just proposing to test this as a science project,” she said. “We’re proposing something that we can very well translate into the clinic and into a new approach for pediatric cancer patients.”
What we hope to discover
Through congressional funding, the Defense Department – one of the largest providers of pediatric healthcare for U.S. children – looks for opportunities to support the needs of military personnel and their dependents. Much of Dr. Haydar’s work will focus on determining safety and optimizing the delivery of the two treatments.
“You have to find the ideal timeline,” Dr. Haydar said. “Which therapy do you do first? How much spacing is best between them, and when do you repeat the therapy? What is the best dosing? It’s a puzzle, and I am hoping to solve it to give children with these often-fatal diagnoses a longer life – and a better one than existing treatments provide.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/05/Haydar-Graphic-LIFU-and-CART-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-05-16 13:58:442024-05-30 18:36:45Mission critical: Pentagon awards grant to combine two novel brain tumor therapies
In a first-of-its-kind clinical trial, researchers found that intravenous therapies made from virus-specific T-cells (VST) can effectively treat immunocompromised pediatric patients, far surpassing the current standard of care, according to new research published in Nature Communications.
More than 60% of patients in the phase 2 clinical trial led by investigators from Children’s National Hospital and Huntsman Cancer Institute responded to the innovative VST therapy. This new treatment uses blood from healthy donors to manufacture a highly specialized immune therapy that, when given to immune-compromised patients, prompts their immune system to fight off potentially life-threatening viruses, including cytomegalovirus, Epstein-Barr and adenovirus. Without this therapy, estimates suggest that less than 30% of patients would recover, using standard protocols.
“A vast majority of our patients not only responded to the therapy, but they were able to come off their antivirals, which come with extensive side effects,” said Michael Keller, M.D., the paper’s first author and the Translational Research Laboratory director at the Children’s National Cell Enhancement and Technologies for Immunotherapy (CETI) program. “This promising data suggests hope for patients with rare immune-compromising diseases that leave them vulnerable to so much in the world.”
The study brings together experts from the Pediatric Transplantation and Cell Therapy Consortium (PTCTC) and the Primary Immune Deficiency Treatment Consortium (PIDTC) to create the first multi-center, pediatric-consortium trial of adoptive T-cell therapies for viruses. It also represents one of the first to include critically ill patients, who are often excluded from research.
Children’s National leads the way
Working alongside Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research (CCIR), Dr. Keller and the CCIR team helped build an internationally recognized program, pioneering therapies to prevent complications from viral infections in immunocompromised patients. This includes patients with congenital immune deficiency and others who have undergone bone marrow transplantation for malignancies or non-malignant conditions, such as sickle cell disease.
While doctors can treat some immune-compromised patients for infections with standard antivirals, a small fraction don’t respond. Children’s National is one of a handful of hospitals in the country that has options. Over the last several decades, researchers have found ways to develop VST therapies made from banked T-cells, a more advanced application of how donated red blood cells are used to treat anemia.
In 2017, Drs. Keller and Bollard started collaborating with Michael Pulsipher, M.D.—now with Intermountain Primary Children’s Hospital and the Huntsman Cancer Institute at the University of Utah—to create a multi-institute clinical study. They combined the expertise at Children’s National in producing and banking cell therapy products with the community built around the PTCTC. Ultimately, they launched a clinical trial that was open to 35 centers in the U.S., enrolling 51 patients at 22 hospitals from 2018-2022.
“We wanted to prove that this potentially life-saving therapy could be given safely at regional pediatric centers that had never been able to use this approach before,” said Dr. Pulsipher, who served as the study’s co-principal investigator with Dr. Keller. “We united top experts in this area from the PTCTC and PIDTC and successfully treated some of the most challenging patients ever treated with this approach. Our findings helped define who can benefit the most from this therapy, paving the way for commercial development.”
The Good Manufacturing Practices (GMP) laboratory at Children’s National, led by Patrick Hanley, Ph.D., provided suitable VST therapies for 75 of 77 patients who requested to join the study. Clinical responses were achieved in 62% of patients who underwent stem cell transplants and in 73% of patients who were treated with VST and evaluated one month after their infusion. The paper laid out risks and clinical factors impacting outcomes when third-party donors are used to manufacture the VST therapies.
What’s ahead
Given that researchers are only beginning to develop cell therapies, work remains to understand the many ways they interact with the immune system. In a separate paper also recently published in Nature Communications, members of the multi-institute team documented a case of an infant with severe combined immune deficiency, who faced extremely rare side effects when the VST treatment interfered with her donor bone marrow graft. The case led the team to work with the Food and Drug Administration to identify criteria for VST donors enrolled in this study to mitigate complications.
In the decade ahead, Dr. Bollard sees promise in cell therapies for patients with cancer, immune deficiencies after transplant and dozens of other disorders, including genetic and autoimmune diseases. “Future studies will continue to look at ways to optimize the manufacturing, the administration and the long-term outcomes for these therapies—and to enhance the lifelong impact on our patients,” she said. “When we pair human ingenuity with the power of technology, I see tremendous potential.”
Acknowledgments: This study was funded with a nearly $5 million grant from the California Institute of Regenerative Medicine and was run through the operations center at the Children’s Hospital of Los Angeles, where Dr. Pulsipher was formerly on faculty.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/04/infusion-featured.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-04-18 14:06:132024-04-18 14:06:13Novel cell therapy treatments offer promise to immune-compromised children
Breakthroughs at the Research & Innovation Campus continued as our researchers worked tirelessly to develop new treatments and therapies that will transform the lives of children and families around the world.
Taking a look at the breakthroughs happening in our now six research centers, we spotlighted the following stories:
Reflecting on decades of progress in the blood, marrow and cell therapy programs at Children’s National. Our researchers have made significant strides in this field, and we are proud to be at the forefront of these life-saving treatments.
In genetic medicine, we continue to be a beacon of hope for families facing rare and complex conditions. Our researchers are making incredible breakthroughs that are changing the landscape of pediatric medicine.
We are also proud to share the $90 million award received from an anonymous donor to support pediatric brain tumor research. The predominant focus of this award is to develop new treatments that will improve outcomes for children with this devastating disease.
This year, we opened a new Center that enhances our research capabilities in the field of Prenatal, Neonatal & Maternal Health Research. We are excited about the possibilities this new center will bring and look forward to the discoveries that will emerge from it.
In addition, we are driving future pandemic readiness with the NIH funded Pediatric Pandemic Network. Our researchers are using cutting-edge technology and innovative approaches to prepare for the next pandemic and protect children.
We are also exploring the potential of artificial intelligence (AI) in pediatric breakthroughs. Our researchers are using machine learning and other AI techniques to develop new treatments and therapies that will transform the lives of children.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/02/2022-2023-Academic-Annual-Report-on-a-computer-CNRI.png385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-02-15 14:18:582024-02-15 15:29:56Driving pediatric breakthroughs through 2023





















 On November 1, Children’s National Hospital installed
On November 1, Children’s National Hospital installed 
 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the 












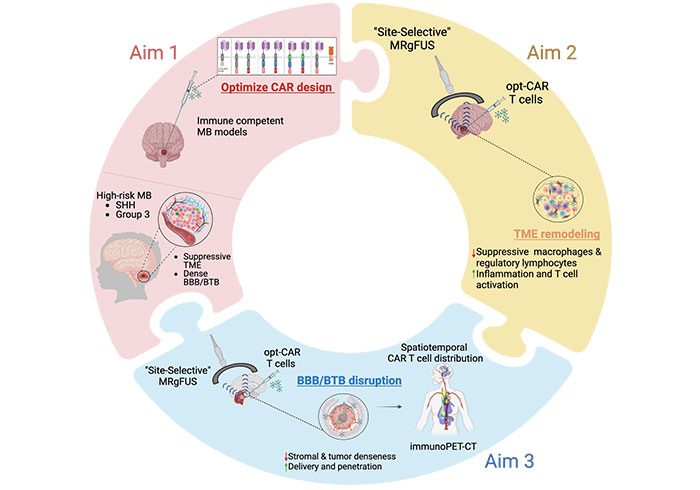 A Children’s National Hospital researcher is embarking on a two-year project that could revolutionize the care of rare pediatric brain tumors, through a Department of Defense (DOD) award to study the efficacy of combining the powers of acoustic therapy and cellular immunotherapy to treat the deadliest forms of medulloblastoma.
A Children’s National Hospital researcher is embarking on a two-year project that could revolutionize the care of rare pediatric brain tumors, through a Department of Defense (DOD) award to study the efficacy of combining the powers of acoustic therapy and cellular immunotherapy to treat the deadliest forms of medulloblastoma.


 The Children’s National Research Institute released its
The Children’s National Research Institute released its 