Children’s National Hospital in Washington, D.C., was ranked in the top 10 nationally in the U.S. News & World Report 2021-22 Best Children’s Hospitals annual rankings. This marks the fifth straight year Children’s National has made the Honor Roll list, which ranks the top 10 children’s hospitals nationwide. In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the fifth year in a row.
For the eleventh straight year, Children’s National also ranked in all 10 specialty services, with seven specialties ranked in the top 10.
“It is always spectacular to be named one of the nation’s best children’s hospitals, but this year more than ever,” says Kurt Newman, M.D., president and CEO of Children’s National. “Every member of our organization helped us achieve this level of excellence, and they did it while sacrificing so much in order to help our country respond to and recover from the COVID-19 pandemic.”
“When choosing a hospital for a sick child, many parents want specialized expertise, convenience and caring medical professionals,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “The Best Children’s Hospitals rankings have always highlighted hospitals that excel in specialized care. As the pandemic continues to affect travel, finding high-quality care close to home has never been more important.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals. The rankings recognize the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News. The top 10 scorers are awarded a distinction called the Honor Roll.
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
Below are links to the seven Children’s National specialty services that U.S. News ranked in the top 10 nationally:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/06/US-NewsTriple-Badge-2021-400x300-1.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-06-15 01:00:392024-12-30 12:48:18For fifth year in a row, Children’s National Hospital nationally ranked a top 10 children’s hospital
The 2021 Pediatric Academic Societies (PAS) Virtual meeting hosted live-streamed events, on-demand sessions with live Q+A, a virtual exhibit hall, poster presentations and networking events that attracted pediatricians and healthcare providers worldwide. Among the physician-scientists, there were over 20 Children’s National Hospital-affiliated participants at this year’s meeting, adding to the conversation of pediatric research in specialty and sub-specialty areas.
Children’s National experts covered a range of topics, including heart disease, neurology, abnormal glycemia in newborns and antibiotic use in hospitalized children.
The “Neurological Implications of Abnormal Glycemia in Neonatal Encephalopathy and Prematurity” was a hot topic symposium presented by a panel of experts, including Sudeepta Basu, M.B.B.S., M.S., neonatologist at Children’s National.
The experts addressed the importance of recognizing early blood glucose disturbances in newborns with encephalopathy following birth asphyxia and its likely impact on brain injury and long-term outcomes. Although whole body cooling for newborns with encephalopathy after birth asphyxia is now standard of care in most advanced centers like Children’s National, many newborns still die or have neurological impairments. Dr. Basu emphasized on the need of continued advances in newer therapies and optimizing intensive care support for these vulnerable newborns immediately after birth. Dr. Basu’s presentation focused on the association of not only low blood glucose (hypoglycemia) but also high blood glucose (hyperglycemia) with abnormal motor, visual and intellectual outcomes in surviving newborns.
“Recognizing the problem is the first step for further advancement,” Dr. Basu said. “The scientific community needs to recognize the importance of early glucose status as an early marker for disease severity and risk of brain injury.” To sum up, Dr. Basu drew attention to recent newborn resuscitation guidelines from the International Liaison Committee on Resuscitation (ILCOR), which recommends close monitoring of blood glucose levels and optimizing supportive care to maintain it within normal range. Dedicated clinical trials are the need of the hour to guide what are “normal” glucose levels in newborns with encephalopathy and what treatment options are most beneficial.
Rana F. Hamdy, M.D., M.P.H., M.S.C.E., director of the Children’s National Antimicrobial Stewardship Program, delved into the increased number of children receiving care for acute conditions – like acute respiratory tract infections – from urgent care centers and direct-to-consumer (DTC) telemedicine companies during her session “Implementing Antibiotic Stewardship in Telemedicine and Urgent Care Settings.”
Telemedicine, in this case, refers to DTC telemedicine companies—not to be confused with the telemedicine established with primary care providers, like the services provided by Children’s National.
There has been little research focused on promoting good antibiotic stewardship in urgent care settings that tend to overprescribe antibiotics compared to a primary care setting. In addition to her work focusing on improving antimicrobial use within Children’s National, Dr. Hamdy has led collaborative quality improvement work nationally in both the pediatric urgent care and DTC telemedicine settings.
“What we’ve learned from our work with the DTC telemedicine setting is that leadership commitment coming from the company is a necessary core element,” Dr. Hamdy said. “There may be unique opportunities in the telemedicine setting to employ the home-grown computer systems for antimicrobial stewardship interventions, for example, incorporating clinical decision support or feedback reports into the electronic health record systems or displaying a commitment letter in the virtual waiting room.”
In the urgent care setting, Dr. Hamdy’s team recruited approximately 150 pediatric urgent care providers to participate in the national quality improvement initiative. Communication training modules for pediatric urgent care providers with scripted language for target infectious conditions — acute otitis media, pharyngitis and otitis media with effusion — were among the successful intervention approaches that led to improved appropriate antibiotic prescribing practices, according to her team’s findings.
“Understanding the prescribing practices in the urgent care setting is important to knowing where and how to focus on target conditions and to be able to support with education and resources,” Dr. Hamdy said. “And understanding the perceived barriers to judicious antibiotic prescribing can help to identify the highest yield interventions.”
This also reflects the approach taken by the outpatient antibiotic stewardship team at the Children’s National Goldberg Center, led by Ariella Slovin, M.D., primary care pediatrics provider at Children’s National Hospital. Dr. Slovin’s oral abstract entitled “Antibiotic Prescribing Via Telemedicine in the Time of COVID-19,” examined the effect that a shift to telemedicine due to the COVID-19 pandemic had on antibiotic use for acute respiratory tract infections. Overall, her team found a decrease in the proportion of acute respiratory tract infections prescribed antibiotics and concluded that the shift to telemedicine did not adversely affect judicious antibiotic prescribing for acute respiratory tract infections.
Other participants from Children’s National included: Taeun Chang, M.D.; Yuan-Chiao Lu, Ph.D.; Chidiogo Anyigbo, M.D., M.P.H.; Panagiotis Kratimenos, M.D.; Sudeepta Basu, M.B.B.S., M.S.; Ashraf Harahsheh, M.D., F.A.C.C., F.A.A.P.; Rana F. Hamdy, M.D., M.P.H., M.S.C.E.; John Idso, M.D.; Michael Shoykhet, M.D., Ph.D.; Monika Goyal, M.D.; Ioannis Koutroulis, M.D., Ph.D., M.B.A.; Josepheen De Asis-Cruz, M.D., Ph.D.; Asad Bandealy, M.D., M.P.H.; Priti Bhansali, M.D.; Sabah Iqbal, M.D.; Kavita Parikh, M.D.; Shilpa Patel, M.D.; Cara Lichtenstein, M.D.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/04/PAS-logo.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-05-10 12:22:362025-02-28 12:29:54Children’s National participants share their expertise at PAS meeting
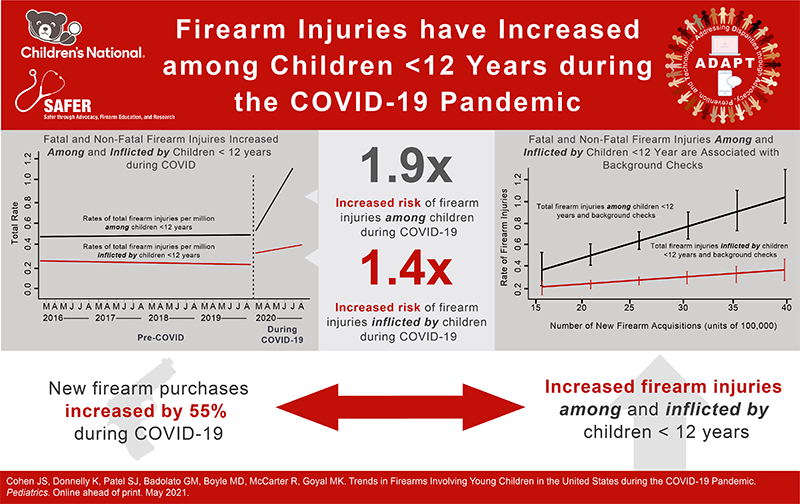
After seeing the surge of firearm injuries in young children and inflicted by young children during the first six months of the COVID-19 pandemic, the study’s experts are saying there is an urgent and critical need for enactment of interventions aimed at preventing firearm injuries and deaths involving children.
A recent study pre-published in Pediatrics found that the COVID-19 pandemic is associated with a surge in fatal and nonfatal firearm injuries both in young children and inflicted by young children, correlating with a rise in firearm acquisitions.
The findings, led by Children’s National Hospital experts, show the risk was higher during the first six months of the COVID-19 pandemic as compared to the pre-COVID period.
“According to the Centers for Disease Control and Prevention, firearms are a leading cause of injury and death among youth,” said Monika K. Goyal, M.D., M.S.C.E., senior author of this study and associate chief of Emergency Medicine and Trauma Services at Children’s National. “The pandemic has led to an increase in these preventable tragedies and it is incumbent upon us as a society to put appropriate measures in place to keep children safe.”
“Increased firearm purchases are one reason we have seen an increase in firearm injuries during the pandemic,” said Joanna S. Cohen, M.D., associate professor of Pediatrics and Emergency Medicine. “Increased purchases are likely related to the political unrest we recently witnessed and increased firearm injuries may be related to children being at home more. Whereas children were in school before, they might be home unsupervised while parents and caretakers are working.”
In addition, there has been an increase in domestic violence over the course of the pandemic which, according to Dr. Cohen, could be a reflection of the stress emerging from financial insecurity, joblessness, illness and other stressors deriving from the pandemic.
After seeing the surge of firearm injuries in young children and inflicted by young children during the first six months of the COVID-19 pandemic, the study’s experts are saying there is an urgent and critical need for enactment of interventions aimed at preventing firearm injuries and deaths involving children.
“There is an urgent need for strategies to prevent further injuries,” Dr. Goyal said. “This includes counseling families on firearm safety at home, having more sensible gun laws and educating the public accordingly.”
In the past, if you were a new gun owner, you would have access to training on how to handle a gun and find safe storage. With all the sheltering in place due to the pandemic, those educational opportunities have fallen by the wayside. “Now you have more people who have become new gun owners but haven’t had the opportunity to get education on safe gun ownership, coinciding with more children staying at home because of the pandemic,” Dr. Goyal said.
The increase in domestic violence could also be a contributing factor. Children are often witnesses to violence at home, Dr. Cohen explained. In many cases, she said, if children see a parent being threatened with a gun, they might model that behavior without fully understanding the implications of holding a gun and the injury it can cause.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/04/Little-boy-going-to-school-with-protective-mask.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-04-13 00:01:162025-09-05 15:49:56Firearm injuries involving young children in the United States during the COVID-19 pandemic
“I’m honored to have been recognized as one of the many women in our city who have worked tirelessly and made a difference during a year that was challenging for so many beyond measure,” Dr. Simpson said.
Joelle Simpson, M.D., medical director of Emergency Preparedness at Children’s National Hospital, received the ‘Washington Woman of Excellence’ 2021 Award from the Mayor Bowser’s Office on Women’s Policy and Initiatives (MOWPI).
Every year, in partnership with the District of Columbia Commission for Women, MOWPI bestow these awards to honor District women who have shown dedication, impact and excellence in the areas of health and wellness, civic engagement and women’s empowerment.
“I’m honored to have been recognized as one of the many women in our city who have worked tirelessly and made a difference during a year that was challenging for so many beyond measure,” Dr. Simpson said.
Dr. Simpson was selected for the Sheroes of Health category.
The distinction of this award is shared with a broad cohort of women who work across all eight wards in Washington D.C. Dr. Simpson was recognized for various of her roles, including her leadership and significant accomplishments as medical director for Emergency Preparedness at Children’s National; her work as an Emergency Department physician leading the D.C. Pediatric Medical Reserves Corps; and for her expertise and leadership in impacting the outcomes for children and the community during COVID-19 health emergency.
The Mayor and members of the DC Commission for Women celebrated the annual Washington Women of Excellence Awards virtually.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/04/Joelle-Simpson.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-04-07 09:06:342021-04-07 09:06:34Joelle Simpson, M.D., receives ‘Washington Woman of Excellence’ 2021 Award
The robot, which is part of the FCC-funded COVID-19 Telehealth Program at Children’s National, is the latest innovation of the program that has rapidly evolved due to the ongoing pandemic.
Children and families who come into the emergency room at Children’s National Hospital may be surprised when their doctor comes in – in the form of a robot. Children’s National introduced a new robot to its Emergency Department (ED) for patients under evaluation for a COVID infection or being treated for other conditions. The robot, which is part of the FCC-funded COVID-19 Telehealth Program at Children’s National, is the latest innovation of the program that has rapidly evolved due to the ongoing pandemic.
“The robot can move in and out of spaces that otherwise we couldn’t get a significant number of providers in, especially with COVID-19 restrictions in place,” said Shireen Atabaki, M.D., M.P.H., associate medical director of Telemedicine, emergency medicine physician and program director for the COVID-19 Telehealth Program at Children’s National. “This is a really exciting program and it implements innovation that we might not have been able to do without the insights we’ve gained from the pandemic.”
The robot is Wi-Fi-enabled and can be remotely controlled by the physician providing the teleconsultation to monitor patient vitals — such as heart rate, body temperature or respiration rate. This allows doctors to work virtually with their team while also having the flexibility to attend to patients faster.
“The pandemic has made us aware of the need to protect patients, families and staff from infectious diseases,” said Alejandro Jose Lopez-Magallon, M.D., medical director of Telemedicine at Children’s National. The robot, he noted, spares clinicians from having to change their PPE, which saves time and gives them the ability to move on to the next patient while nurses and staff continue to provide bedside care.
“We have also seen that whenever a remote clinician is completely alone in the command center and can get on-screen without a mask, in a paradoxical way our patients may be more accepting of seeing a face on a screen that’s not covered with a mask and shield than a stranger using a mask in the same room,” Dr. Lopez-Magallon added.
Soon, the robot will also be used to coordinate subspecialty care — such as cardiac care — in the ED. This will provide more streamlined and expedited care for patients. Instead of leaving with a referral to set up a follow-up appointment with a specialist, patients would be able to receive the consult they need during the same appointment.
The robot is also presenting promising solutions for concerns around the number of restricted visitors. The team at Children’s National recently piloted using an iPad and other technology purchased with the FCC funds to remotely connect family members with patients.
“We downloaded the Zoom app to iPads in our ED to be able to coordinate calls between family members who can’t come in and see patients,” said Dr. Atabaki. “We are looking to implement this as a permanent solution keeping in mind how burdensome and emotionally stressful it has been for many not having the ability to be by the loved one’s side during such a challenging time.”
The FCC funds also covered the telehealth carts, tablets and other connected devices, the telehealth platform, telehealth equipment and innovative AI (augmented intelligence) to treat seriously ill COVID-19 pediatric patients.
The emergency department robot brings the robot-fleet at Children’s National up to three. The first robot was debuted in 2019 to serve children and families in the Cardiac Intensive Care Unit.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/04/ED-robot.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-04-06 12:00:182021-04-06 12:33:42New robot helps care for kids in the emergency room at Children’s National Hospital
Formal training in academic pediatric urgent care is a relatively new concept, but it is one that is rapidly gaining popularity due to consumer demand for low-cost convenient care.
As of 2017, there were 7,639 urgent care centers in the United States, with 21% dedicated to the treatment of pediatric patients. This rapid growth of urgent care centers has resulted in an increased need for urgent care providers, and has led to the development of fellowships focused on efficient evidence-based urgent care management.
In an article published in the Journal of Pediatrics, Deena D. Berkowitz, M.D., M.P.H., medical director of Fast Track Services and co-director of the Children’s National Hospital Urgent Care Fellowship, and Haroon Shaukat, M.D., assistant program director of the Children’s National Hospital Urgent Care Fellowship, and their colleagues summarized the current state and future direction formal training in academic pediatric urgent care. The authors conclude that “systematic training in acute ambulatory pediatric care will advance high quality clinical care and research on patient care, scope, and outcomes in pediatric urgent care.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/01/Pediatrician-talking-with-young-girl.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-01-12 10:56:392021-01-15 10:39:04The current state of academic pediatric urgent care fellowships
“The past year has been a stark reminder about the importance of partnership and working together toward common goals,” says Dr. Beers. “I am humbled and honored to be taking on this role at such a pivotal moment for the future health and safety of not only children, but the community at large.”
Lee Savio Beers, M.D., F.A.A.P., medical director of Community Health and Advocacy at the Child Health Advocacy Institute (CHAI) at Children’s National Hospital, has begun her term as president of the American Academy of Pediatrics (AAP). The AAP is an organization of 67,000 pediatricians committed to the optimal physical, mental and social health and well-being for all children – from infancy to adulthood.
“The past year has been a stark reminder about the importance of partnership and working together toward common goals,” says Dr. Beers. “I am humbled and honored to be taking on this role at such a pivotal moment for the future health and safety of not only children, but the community at large.”
Dr. Beers has pledged to continue AAP’s advocacy and public policy efforts and to further enhance membership diversity and inclusion. Among her signature issues:
Partnering with patients, families, communities, mental health providers and pediatricians to co-design systems to bolster children’s resiliency and to alleviate growing pediatric mental health concerns.
Continuing to support pediatricians during the COVID-19 pandemic with a focus on education, pediatric practice support, vaccine delivery systems and physician wellness.
Dr. Beers is looking forward to continuing her work bringing together the diverse voices of pediatricians, children and families as well as other organizations to support improving the health of all children.
“Dr. Beers has devoted her career to helping children,” says Kurt Newman, M.D., president and chief executive officer of Children’s National. “She has developed a national advocacy platform for children and will be of tremendous service to children within AAP national leadership.”
Read more about Dr. Beer’s career and appointment as president of the AAP.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/09/Lee-Beers.jpg400300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-01-04 11:10:372025-12-08 16:45:25Lee Beers, M.D., F.A.A.P, begins term as AAP president
A new study looking at the results of testing children for COVID-19 through a Children’s National Hospital community-based testing site found that one in four patients had a positive test.
A new study looking at the results of testing children for COVID-19 through a Children’s National Hospital community-based testing site found that one in four patients had a positive test. The findings, reported online Dec. 18 in The Journal of Pediatrics, reinforce that children and young adults are impacted by the virus more than originally believed, and that the continued understanding of their role in transmitting COVID-19 is essential to getting the virus under control.
Of the 1,445 patients tested at the specimen collection site for SARS-CoV-2 virus between March 21 and May 16, 2020, the median age was 8 years old, and more than 34% of positive patients were Hispanic, followed by non-Hispanic Black and non-Hispanic white. The daily positivity rate increased over the study period, from 5.4% during the first week to a peak of 47.4% in May. Children and adolescents were referred to the testing site because of risk of exposure or mild symptoms.
“We knew that community-based testing sites were key in minimizing exposure risk to other patients and health care workers, preserving PPE, centralizing specimen collection services, mitigating acute care site overcrowding and informing our community of the burden caused by this disease,” says Joelle Simpson, M.D., medical director of Emergency Preparedness at Children’s National.
Drive-through/walk-up testing sites outside of a traditional acute care setting have emerged around the world to meet the need for testing mildly ill or asymptomatic individuals. In March, Children’s National Hospital opened a drive-up/walk-up location — one of the first exclusively pediatric testing sites for the virus in the U.S. — where primary care doctors in the Washington, D.C., region could refer young patients for COVID-19 specimen collection and testing.
“At first, children were not the target of testing initiatives, but it is clear that making testing available to pediatric patients early was a very important part of the pandemic response,” says Meghan Delaney, D.O., M.P.H., chief of Pathology and Laboratory Medicine at Children’s National. “Not only can children get severe disease, they can be part of positive clusters with the adults they live with. The knowledge we have gained by testing many thousands of children over the pandemic has provided key information.”
Compared with non-Hispanic white children and after adjustments for age, sex and distance of residence from specimen collection site, minority children had a higher likelihood of infection.
“We wanted to identify the features of children tested at this site who did not require acute medical care and be able to compare demographic and clinical differences between patients who tested positive and negative for COVID-19,” says Dr. Simpson.
Patients with COVID-19 exposure and symptoms were more likely to have a positive test than patients without symptoms. This supports contact tracing for symptomatic cases and testing as an important tool in detecting and containing community spread, according to the study’s findings. Although most patients were referred because they lived with a family member with high risk for exposure or infection, this was not associated with positive test results.
“The impact of this virus is broad and affects planning for children, especially as schools and childcare centers work to reopen,” Dr. Simpson says. “In order to guide the development of measures to control the ongoing pandemic, we need better understand the transmission potential of these mildly symptomatic or well children and young adults.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/12/Medical-professional-taking-a-nasal-swab-of-child.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-12-21 13:59:292020-12-21 13:59:29COVID testing results highlight importance of understanding virus in children
Drs. Dewesh Agrawal, Andrew Dauber, Robert Freishtat and Vittorio Gallo were named as 2021 American Pediatric Society members.
The American Pediatric Society (APS) has announced 55 new members, four of which are experts from Children’s National Hospital. Founded in 1888, the APS is the first and most prestigious academic pediatric organization in North America.
APS members are recognized child health leaders of extraordinary achievement who work together to shape the future of academic pediatrics. New members are nominated by current members through a process that recognizes individuals who have distinguished themselves as child health leaders, teachers, scholars, policymakers and/or clinicians.
“Our members represent the most distinguished and accomplished academic leaders in pediatrics whose outstanding work has advanced child health,” said APS President Steven Abman, M.D. “I am honored to welcome this exceptional group of individuals to the APS. The APS is especially looking forward to the active engagement of our membership with many exciting programs within the organization that are directed towards improvements in academic pediatric medicine, including more vigorous approaches to express our values of anti-racism, equity, diversity and inclusion.”
APS 2021 active new members from Children’s National are:
Dewesh Agrawal, M.D., vice-chair for Medical Education at Children’s National. Agrawal’s career has been marked by academic honors and teaching awards at every stage of his training and faculty employment. He has relentlessly devoted his energy to improving the educational experience for students, residents and fellows at Children’s National.
Andrew Dauber, M.D., M.M.Sc., chief of Endocrinology at Children’s National. Dr. Dauber’s leadership is reflected, nationally and internationally, in his ability to create research consortia, bringing together investigators to tackle complex questions. For example, he leads an NIH-funded consortium on the genetics of short statures, with multiple top children’s hospitals as partners. He also leads a large clinical trial testing a novel therapeutic agent for genetic short stature.
Robert Freishtat, M.D., M.P.H., senior investigator in the Center for Genetic Medicine of the Children’s National Research Institute (CNRI). Dr. Freishtat has authored or co-authored more than 100 articles and book chapters in the fields of pediatric lung injury, asthma, obesity, exosomes and emergency medicine. His research has been continuously funded by the NIH since 2003.
Vittorio Gallo, Ph.D., chief research officer at Children’s National and scientific director of CNRI. Dr. Gallo’s scientific success is attested to by over 130 peer-reviewed publications, many in very high-profile journals, as well as over 30 review articles and book chapters. He has received many national and international awards, including the NINDS Javits award in Neuroscience in 2018. Dr. Gallo has served on the editorial boards of many neuroscience journals, including Glia and the Annual Review in Neuroscience, and has been reviewing editor for the Journal of Neuroscience, all of which is a testament to the tremendous impact that his studies have had on the advancement of neurosciences.
“These new members represent multiple areas of Children’s National and have all leveraged the intersection of science, medicine and clinical education to make advances in their field of study,” said Stephen J. Teach, M.D., M.P.H., chair of the Department of Pediatrics at Children’s National. “Their work has, and will continue to, advance pediatric health care, and I congratulate them on their APS membership.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/12/APS-Members-2021.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-12-01 15:02:332024-11-27 09:44:31Four Children’s National Hospital leaders named to APS
Black and Hispanic adolescents are significantly more likely to die from shootings related to police intervention compared to non-Hispanic white adolescents, a recent study shows.
A recent study evaluating the use of force by police against children found that Black and Hispanic adolescents are significantly more likely to die from shootings related to police intervention compared to non-Hispanic white adolescents. The findings, led by Children’s National Hospital researchers and reported online Nov. 24 in Pediatrics, mirror similar racial and ethnic disparities in adults and highlight the need for interventions and policies to mitigate these tragedies.
In recent years, concerns about police use of force — particularly its disproportionate application to people of color — have grown exponentially in the U.S. Between 2003 and 2018, there were 6,512 firearm deaths from police intervention in adults, with non-Hispanic Blacks and Hispanics having significantly higher per population mortality rates than whites. However, it’s been unclear whether similar racial and ethnic disparities exist for adolescents killed by police intervention.
To explore this question, Monika K. Goyal, M.D., M.S.C.E., associate division chief of Emergency Medicine and Trauma Services and director of Academic Affairs and Research at Children’s National, and her colleagues used data from the Centers for Disease Control and Prevention’s Web-Based Injury Statistics Query and Reporting System. This database collects national data from death certificates compiled by the National Center for Health Statistics, including cause of death and race and ethnicity.
The researchers identified all adolescents between the ages of 12 and 17 years of age who died from firearm injuries due to police intervention between 2003 and 2018 within this database. They then compared rates of these deaths across different racial and ethnic populations based on U.S. Census Bureau data.
Dr. Goyal and her colleagues found that during the 16-year study period, 140 adolescents had died from police intervention, and of those, 113 involved firearms. The vast majority — about 93% — were male, with a mean age of about 16 years.
Using census data, the researchers found that the rate of firearm deaths due to police intervention was markedly higher among non-Hispanic Black and Hispanic youth when compared to non-Hispanic white youth. Numbers show that, compared to non-Hispanic white children, non-Hispanic Black children had a six-fold higher risk of death due to legal intervention. Similarly, Hispanic children had a risk of death almost three times higher.
“As the country works to reform policing practices and strives to mitigate disparities in our justice system, it is essential we do not forget the disproportionate impact on children of color,” Dr. Goyal says. “Our study confirms these disparities that are stark and unacceptable.”
Dr. Goyal adds that the study only collected data on adolescents who died, rather than non-fatal shootings, and thus, may underestimate the true toll of disparities in use of firearms against youth due to police intervention. Although the study was not designed to investigate the causes of these disparities, she says, recent events provide evidence of structural racism and bias among law enforcement personnel and in its policies.
Although these numbers are small, Dr. Goyal notes that there’s a potential rippling effect, with the death of each child having wide-ranging impact on an entire community.
“Any death of a child is devastating but when it is due to police violence, it leads to distrust in the system and undermines the primary mission to protect,” she says. “The pattern of stark racial and ethnic disparities only adds to this tragedy, further oppressing and alienating communities of color. It’s important to investigate, identify and correct those policies and personnel that perpetuate and exacerbate these disparities.”
Other researchers who contributed to this study include Gia M. Badolato, M.P.H., Meleah D. Boyle, M.P.H., and Robert McCarter, Sc.D., all of Children’s National; April M. Zeoli of Michigan State University; and William Terrill of Arizona State University.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/11/Motion-blur-ambulance.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-11-24 10:09:302021-10-04 08:36:13Racial disparities in pediatric deaths related to police intervention
Children’s National Hospital announced a $5 million gift from The Boeing Company that will help drive lifesaving pediatric discoveries at the new Children’s National Research & Innovation Campus.
Children’s National Hospital announced a $5 million gift from The Boeing Company that will help drive lifesaving pediatric discoveries at the new Children’s National Research & Innovation Campus. The campus, now under construction, is being developed on nearly 12 acres of the former Walter Reed Army Medical Center. Children’s National will name the main auditorium in recognition of Boeing’s generosity.
“We are deeply grateful to Boeing for their support and commitment to improving the health and well-being of children in our community and around the globe,” said Kurt Newman, M.D., president and CEO of Children’s National “The Boeing Auditorium will help the Children’s National Research & Innovation campus become the destination for discussion about how to best address the next big healthcare challenges facing children and families.”
The one-of-a-kind pediatric hub will bring together public and private partners for unprecedented collaborations. It will accelerate the translation of breakthroughs into new treatments and technologies to benefit kids everywhere.
“Children’s National Hospital’s enduring mission of positively impacting the lives of our youngest community members is especially important today,” said Boeing President and CEO David Calhoun. “We’re honored to join other national and community partners to advance this work through the establishment of their Research & Innovation Campus.”
Children’s National Research & Innovation Campus partners currently include Johnson & Johnson Innovation – JLABS, Virginia Tech, the National Institutes of Health (NIH), Food & Drug Administration (FDA), U.S. Biomedical Advanced Research and Development Authority (BARDA), Cerner, Amazon Web Services, Microsoft, National Organization of Rare Diseases (NORD) and local government.
The 3,200 square-foot Boeing Auditorium will be the focal point of the state-of-the-art conference center on campus. Nationally renowned experts will convene with scientists, medical leaders and diplomats from around the world to foster collaborations that spur progress and disseminate findings.
Boeing’s $5 million commitment deepens its longstanding partnership with Children’s National. The company has donated nearly $2 million to support pediatric care and research at Children’s National through Chance for Life and the hospital’s annual Children’s Ball. During the coronavirus pandemic, Boeing fabricated and donated 2,000 face shields to help keep patients and frontline care providers at Children’s National safe.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/02/Research-Innovation-Campus.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-11-05 11:16:312023-07-03 10:40:51Boeing gives $5 million to support Research & Innovation Campus
Children’s National Hospital is the first pediatric partner to join an international initiative led by leading technology firm NVIDIA and Massachusetts General Brigham Hospital, focused on creating solutions through machine and deep learning to benefit COVID-19 healthcare outcomes.
Children’s National Hospital is the first pediatric partner to join an international initiative led by leading technology firm NVIDIA and Massachusetts General Brigham Hospital, focused on creating solutions through machine and deep learning to benefit COVID-19 healthcare outcomes. The initiative, known as EXAM (EMR CXR AI Model) is the largest and most diverse federated learning enterprise, comprised of 20 leading hospitals from around the globe.
“Children’s National Hospital is proud to be the first pediatric partner joining the world’s leading healthcare institutions in this collaboration to advance global health,” says Linguraru. “We are currently living in a time where rapid access to this kind of global data has never been more important — we need solutions that work fast and are effective. That is not possible without this degree of collaboration and we look forward to continuing this important work with our partners to address one of the most significant healthcare challenges in our lifetime.”
A recent systematic review and meta-analysis from Children’s National Hospital became another core contribution to understanding how children are impacted by COVID-19. Led by Linguraru and accepted to be published in Pediatric Pulmonology, it offers the first comprehensive summary of the findings of various studies published thus far that describe COVID-19 lung imaging data across the pediatric population.
The review examined articles based on chest CT imaging in 1,026 pediatric patients diagnosed with COVID-19, and concluded that chest CT manifestations in those patients could potentially be used to prompt intervention across the pediatric population.
“Children’s National Hospital is proud to be the first pediatric partner joining the world’s leading healthcare institutions in this collaboration to advance global health,” says Marius George Linguraru, D.Phil., M.A., M.Sc.
“Until this point, pediatric COVID-19 studies have largely been restricted to case reports and small case series, which have prevented the identification of any specific pediatric lung disease patterns in COVID-19 patients,” says Linguraru. “Not only did this review help identify the common patterns in the lungs of pediatric patients presenting COVID-19 symptoms, which are distinct from the signs of other viral respiratory infections in children, it also provided insight into the differences between children and adults with COVID-19.”
Earlier this month, NVIDIA announced the EXAM initiative had – in just 20 days – developed an artificial intelligence (AI) model to determine whether a patient demonstrating COVID-19 symptoms in an emergency room would require supplemental oxygen hours – even days – after the initial exam. This data ultimately aids physicians in determining the proper level of care for patients, including potential ICU placement.
The EXAM initiative achieved a machine learning model offering precise prediction for the level of oxygen incoming patients would require.
In addition to Children’s National Hospital, other participants included Mass Gen Brigham and its affiliated hospitals in Boston; NIHR Cambridge Biomedical Research Centre; The Self-Defense Forces Central Hospital in Tokyo; National Taiwan University MeDA Lab and MAHC and Taiwan National Health Insurance Administration; Tri-Service General Hospital in Taiwan; Kyungpook National University Hospital in South Korea; Faculty of Medicine, Chulalongkorn University in Thailand; Diagnosticos da America SA in Brazil; University of California, San Francisco; VA San Diego; University of Toronto; National Institutes of Health in Bethesda, Maryland; University of Wisconsin-Madison School of Medicine and Public Health; Memorial Sloan Kettering Cancer Center in New York; and Mount Sinai Health System in New York.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/10/communication-network-concept-illustration.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-10-28 10:49:012020-10-28 10:49:01Children’s National joins international AI COVID-19 initiative
Children’s National Hospital in Washington, D.C., was ranked No. 7 nationally in the U.S. News & World Report 2020-21 Best Children’s Hospitals annual rankings. This marks the fourth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide.
In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the fourth year in a row.
For the tenth straight year, Children’s National also ranked in all 10 specialty services, with seven specialties ranked in the top 10.
“Our number one goal is to provide the best care possible to children. Being recognized by U.S. News as one of the best hospitals reflects the strength that comes from putting children and their families first, and we are truly honored,” says Kurt Newman, M.D., president and CEO of Children’s National Hospital.
“This year, the news is especially meaningful, because our teams — like those at hospitals across the country — faced enormous challenges and worked heroically through a global pandemic to deliver excellent care.”
“Even in the midst of a pandemic, children have healthcare needs ranging from routine vaccinations to life-saving surgery and chemotherapy,” said Ben Harder, managing editor and chief of Health Analysis at U.S. News. “The Best Children’s Hospitals rankings are designed to help parents find quality medical care for a sick child and inform families’ conversations with pediatricians.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals. The rankings recognize the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News. The top 10 scorers are awarded a distinction called the Honor Roll.
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
Below are links to the seven Children’s National specialty services that U.S. News ranked in the top 10 nationally:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/06/US-News-2020-ID.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-06-16 01:00:292024-12-30 12:50:15Children’s National ranked a top 10 children’s hospital and No. 1 in newborn care nationally by U.S. News
Children’s National Research Institute directors Vittorio Gallo, Ph.D., and Mark Batshaw, M.D.
The Children’s National Research Institute recently released its 2019-2020 academic annual report, titled 150 Years Stronger Through Discovery and Care to mark the hospital’s 150th birthday. Not only does the annual report give an overview of the institute’s research and education efforts, but it also gives a peek in to how the institute has mobilized to address the coronavirus pandemic.
“Our inaugural research program in 1947 began with a budget of less than $10,000 for the study of polio — a pressing health problem for Washington’s children at the time and a pandemic that many of us remember from our own childhoods,” says Vittorio Gallo, Ph.D., chief research officer at Children’s National Hospital and scientific director at Children’s National Research Institute. “Today, our research portfolio has grown to more than $75 million, and our 314 research faculty and their staff are dedicated to finding answers to many of the health challenges in childhood.”
Highlights from the Children’s National Research Institute annual report
In 2018, Children’s National began construction of its new Research & Innovation Campus (CNRIC) on 12 acres of land transferred by the U.S. Army as part of the decommissioning of the former Walter Reed Army Medical Center campus. In 2020, construction on the CNRIC will be complete, and in 2012, the Children’s National Research Institute will begin to transition to the campus.
In late 2019, a team of scientists led by Eric Vilain, M.D., Ph.D., director of the Center for Genetic Medicine Research, traveled to the Democratic Republic of Congo to collect samples from 60 individuals that will form the basis of a new reference genome data set. The researchers hope their project will generate better reference genome data for diverse populations, starting with those of Central African descent.
A gift of $5.7 million received by the Center for Translational Research’s director, Lisa Guay-Woodford, M.D., will reinforce close collaboration between research and clinical care to improve the care and treatment of children with polycystic kidney disease and other inherited renal disorders.
The Center for Neuroscience Research’s integration into the infrastructure of Children’s National Hospital has created a unique set of opportunities for scientists and clinicians to work together on pressing problems in children’s health.
Children’s National and the National Institute of Allergy and Infectious Diseases are tackling pediatric research across three main areas of mutual interest: primary immune deficiencies, food allergies and post-Lyme disease syndrome. Their shared goal is to conduct clinical and translational research that improves what we know about those conditions and how we care for children who have them.
An immunotherapy trial has allowed a little boy to be a kid again. In the two years since he received cellular immunotherapy, Matthew has shown no signs of a returning tumor — the longest span of time he’s been tumor-free since age 3.
In the past 6 years, the 104 device projects that came through the National Capital Consortium for Pediatric Device Innovation accelerator program raised $148,680,256 in follow-on funding.
Even though he’s watched more than 500 aspiring physicians pass through the Children’s National pediatric residency program, program director Dewesh Agrawal, M.D., still gets teary at every graduation.
Understanding and treating the novel coronavirus (COVID-19)
In a short period of time, Children’s National Research Institute has mobilized its scientists to address COVID-19, focusing on understanding the virus and advancing solutions to ameliorate the impact today and for future generations. Children’s National Research Institute Director Mark Batshaw, M.D., highlighted some of these efforts in the annual report:
Eric Vilain, M.D., Ph.D., director of the Center for Genetic Medicine Research, is looking at whether or not the microbiome of bacteria in the human nasal tract acts as a defensive shield against COVID-19.
Catherine Bollard, M.D., MBChB, director of the Center for Cancer and Immunology Research, and her team are seeing if they can “train” T cells to attack the invading coronavirus.
Sarah Mulkey, M.D., Ph.D., an investigator in the Center for Neuroscience Research and the Fetal Medicine Institute, is studying the effects of, and possible interventions for, coronavirus on the developing brain.
You can view the entire Children’s National Research Institute academic annual report online.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/05/Vittorio-Gallo-and-Marc-Batshaw.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-05-19 14:08:392024-06-28 13:19:46Children’s National Research Institute releases annual report
After a teen was transferred to Children’s National Hospital suffering from severe difficulty breathing and swallowing, a multidisciplinary team continued the detective work and surmises that vaping was to blame for her unusual symptoms.
A teenage girl with no hint of prior asthma or respiratory illness began to feel hoarseness in her throat and a feeling that she needed to clear her throat frequently. Within a few weeks, her hoarseness and throat-clearing worsened with early morning voice loss and feeling as if food were lodged in her throat. She started having trouble swallowing and began to avoid food all together.
Her pediatrician prescribed loratadine for suspected allergies to no avail. Days later, an urgent care center prescribed a three-day course of prednisone. For a few days, she felt a little better, but went back to feeling like she was breathing “through a straw.” After going to an emergency room with acute respiratory distress and severe difficulty swallowing, staff tried intravenous dexamethasone, ampicillin/sulbactam, and inhaled racemic epinephrine and arranged for transfer.
When she arrived at Children’s National Hospital, a multidisciplinary team continued the detective work with additional testing, imaging and bloodwork.
Examining her throat confirmed moderate swelling and a partially obstructed airway draped with thick chartreuse-colored mucus. The teen had no history of an autoimmune disorder, no international travel and no exposure to animals. She had no fever and had received all her scheduled immunizations.
“With epiglottitis – an inflammation of the flap found at the base of the tongue that prevents food from entering the trachea – our first concern is that an underlying infection is to blame,” says Michael Jason Bozzella, D.O., MS, a third-year infectious diseases fellow and lead author of the case report published Feb. 5, 2020, in Pediatrics. “We tested her specimens in a number of ways for a host of respiratory pathogens, including human rhino/enterovirus, respiratory syncytial virus, influenza, Epstein-Barr virus, Streptococcus and more. All negative. We also looked for more atypical infections with bacteria, like Arcanobacterium, Mycoplasma and Gonorrhea. Those were all negative as well,” Dr. Bozzella adds.
She slowly improved during a seven-day initial hospital stay, though soon returned for another six-day hospital stay after it again became excruciatingly painful for her to swallow.
Every throat culture and biopsy result showed no evidence of fungal, bacterial or viral infection, acid-fast bacilli or other malignancy. But in speaking with doctors, the teen had admitted to using candy-and fruit-flavored e-cigarettes three to five times with her friends over the two months preceding her symptoms. The last time she vaped was two weeks before her unusual symptoms began.
According to the Centers for Disease Control and Prevention, 2,668 people in the U.S. have been hospitalized for e-cigarette or vaping product use-associated lung injury, as of Jan. 14, 2020. The Children’s National case report’s authors say the increasing use of vaping products by teenagers highlights the potential for unknown health risks to continue to grow.
“This teenager’s use of e-cigarettes is the most plausible reason for this subacute epiglottitis diagnosis, a condition that can become life-threatening,” says Kathleen Ferrer, M.D., a hospitalist at Children’s National and the case report’s senior author. “This unusual case adds to a growing list of toxic effects attributable to vaping. While we normally investigate infectious triggers, like Streptococci, Staphylococci and Haemophilus, we and other health care providers should also consider e-cigarettes as we evaluate oro-respiratory complaints.”
Recently, Kurt Newman, M.D., president and CEO of Children’s National Hospital, authored an opinion piece for the popular political website, The Hill. In the article, he called upon stakeholders from across the landscape to address the significant innovation gap in children’s healthcare versus adults.
As Chair of the Board of Trustees of the Children’s Hospital Association, Dr. Newman knows the importance of raising awareness among policy makers at the federal and state level about the healthcare needs of children. Dr. Newman believes that children’s health should be a national priority that is addressed comprehensively. With years of experience as a pediatric surgeon, he is concerned by the major inequities in the advancements of children’s medical devices and technologies versus those for adults. That’s why Children’s National is working to create collaborations, influence policies and facilitate changes that will accelerate the pace of pediatric healthcare innovation for the benefit of children everywhere. One way that the hospital is tackling this challenge is by developing the Children’s National Research & Innovation Campus, which will be the nation’s first innovation campus focused on pediatric research.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/02/Kurt-Newman-capitol-building.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2019-12-11 15:41:002023-07-10 10:07:22Making healthcare innovation for children a priority
Children’s National Hospital and Virginia Tech create formal partnership that includes the launch of a Virginia Tech biomedical research facility within the new Children’s National Research & Innovation Campus.
Children’s National Hospital and Virginia Tech recently announced a formal partnership that will include the launch of a 12,000-square-foot Virginia Tech biomedical research facility within the new Children’s National Research & Innovation Campus. The campus is an expansion of Children’s National that is located on a nearly 12-acre portion of the former Walter Reed Army Medical Center in Washington, D.C. and is set to open its first phase in December 2020. This new collaboration brings together Virginia Tech, a top tier academic research institution, with Children’s National, a U.S. News and World Report top 10 children’s hospital, on what will be the nation’s first innovation campus focused on pediatric research.
“Virginia Tech is an ideal partner to help us deliver on what we promised for the Children’s National Research & Innovation Campus – an ecosystem that enables us to accelerate the translation of potential breakthrough discoveries into new treatments and technologies,” says Kurt Newman, M.D., president and CEO, Children’s National. “Our clinical expertise combined with Virginia Tech’s leadership in engineering and technology, and its growing emphasis on biomedical research, will be a significant advance in developing much needed treatment and cures to save children’s lives.”
Earlier this year, Children’s National announced a collaboration with Johnson & Johnson Innovation LLC to launch JLABS @ Washington, DC at the Research & Innovation Campus. The JLABS @ Washington, DC site will be open to pharmaceutical, medical device, consumer and health technology companies that are aiming to advance the development of new drugs, medical devices, precision diagnostics and health technologies, including applications in pediatrics.
“We are proud to welcome Virginia Tech to our historic Walter Reed campus – a campus that is shaping up to host some of the top minds, talent and innovation incubators in the world,” says Washington, D.C. Mayor Muriel Bowser. “The new Children’s National Research & Innovation Campus will exemplify why D.C. is the capital of inclusive innovation – because we are a city committed to building the public and private partnerships necessary to drive discoveries, create jobs, promote economic growth and keep D.C. at the forefront of innovation and change.”
Faculty from the Children’s National Research Institute and the Fralin Biomedical Research Institute at Virginia Tech Carilion (VTC) have worked together for more than a decade, already resulting in shared research grants, collaborative publications and shared intellectual property. Together, the two institutions will now expand their collaborations to develop new drugs, medical devices, software applications and other novel treatments for cancer, rare diseases and other disorders.
“Joining with Children’s National in the nation’s capital positions Virginia Tech to improve the health and well-being of infants and children around the world,” says Virginia Tech President Tim Sands, Ph.D. “This partnership resonates with our land-grant mission to solve big problems and create new opportunities in Virginia and D.C. through education, technology and research.”
The partnership with Children’s National adds to Virginia Tech’s growing footprint in the Washington D.C. region, which includes plans for a new graduate campus in Alexandria, Va. with a human-centered approach to technological innovation. Sands said the proximity of the two locations – just across the Potomac – will enable researchers to leverage resources, and will also create opportunities with the Virginia Tech campus in Blacksburg, Va. and the Virginia Tech Carilion Health Science and Technology campus in Roanoke, Va.
Carilion Clinic and Children’s National have an existing collaboration for provision of certain specialized pediatric clinical services. The more formalized partnership between Virginia Tech and Children’s National will drive the already strong Virginia Tech-Carilion Clinic partnership, particularly for children’s health initiatives and facilitate collaborations between all three institutions in the pediatric research and clinical service domains.
Children’s National and Virginia Tech will engage in joint faculty recruiting, joint intellectual property, joint training of students and fellows, and collaborative research projects and programs according to Michael Friedlander, Ph.D., Virginia Tech’s vice president for health sciences and technology, and executive director of the Fralin Biomedical Research Institute at VTC.
“The expansion and formalization of our partnership with Children’s National is extremely timely and vital for pediatric research innovation and for translating these innovations into practice to prevent, treat and ultimately cure nervous system cancer in children,” says Friedlander, who has collaborated with Children’s National leaders and researchers for more than 20 years. “Both Virginia Tech and Children’s National have similar values and cultures with a firm commitment to discovery and innovation in the service of society.”
“Brain and other nervous system cancers are among the most common cancers in children (alongside leukemia),” says Friedlander. “With our strength in neurobiology including adult brain cancer research in both humans and companion animals at Virginia Tech and the strength of Children’s National research in pediatric cancer, developmental neuroscience and intellectual disabilities, this is a perfect match.”
The design of the Children’s National Research & Innovation Campus not only makes it conducive for the hospital to strengthen its prestigious partnerships with Virginia Tech and Johnson & Johnson, it also fosters synergies with federal agencies like the Biomedical Advanced Research and Development Authority, which will collaborate with JLABS @ Washington, DC to establish a specialized innovation zone to develop responses to health security threats. As more partners sign on, this convergence of key public and private institutions will accelerate discoveries and bring them to market faster for the benefit of children and adults.
“The Children’s National Research & Innovation Campus pairs an inspirational mission to find new treatments for childhood illness and disease with the ideal environment for early stage companies. I am confident the campus will be a magnet for big ideas and will be an economic boost for Washington DC and the region,” says Jeff Zients, who was appointed chair of the Children’s National Board of Directors effective October 1, 2019. As a CEO and the former director of President Obama’s National Economic Council, Zients says that “When you bring together business, academia, health care and government in the right setting, you create a hotbed for innovation.”
Ranked 7th in National Institutes of Health research funding among pediatric hospitals, Children’s National continues to foster collaborations as it prepares to open its first 158,000-square-foot phase of its Research & Innovation Campus. These key partnerships will enable the hospital to fulfill its mission of keeping children top of mind for healthcare innovation and research while also contributing to Washington D.C.’s thriving innovation economy.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/12/VT_CNRICampus_Rendering-sm.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2019-12-11 10:18:202023-07-03 10:40:18Children’s National welcomes Virginia Tech to its new campus
Lenore Jarvis, M.D., MEd, FAAP, will participate in a symposium of surgeons, neurosurgeons and emergency medicine doctors during the American Academy of Pediatrics National Conference and Exhibition – the first time these groups have come together to help reduce the number of kids hurt or killed by firearms.
Lenore Jarvis, M.D., MEd, FAAP, remembers feeling fatigue and frustration when, despite her team’s herculean efforts, a 5-year-old died from accidental gunshot wounds. The preschooler had been feeling playful: He surprised a family member who mistook him for an intruder and fired, fatally wounding the child.
As an Emergency Medicine and Trauma Services specialist at Children’s National Hospital, Dr. Jarvis has cared for kids with a range of firearm-related injuries from accidental shootings, intentional acts of violence or suicide attempts. Even when children survive such traumatic injuries, their lives are indelibly altered.
“We’re trained to save lives, but we also want to prevent childhood injuries, if possible. As I considered this young child’s life ending so prematurely and so tragically, I thought I should do more. I could do more,” recalls Dr. Jarvis, the division’s director of advocacy and health policy.
To that end, in addition to advocacy at the regional and national level, on Oct. 26, 2019, Dr. Jarvis will participate in a four-hour symposium of surgeons, neurosurgeons and emergency medicine doctors during the American Academy of Pediatrics (AAP) National Conference and Exhibition – the first time these groups have come together to explore ways they can help to reduce the number of kids hurt or killed by firearms.
Dr. Jarvis will set the stage for the day’s collective call to action when she counsels pediatricians about how they can advocate within the clinic by simple actions such as:
Asking families if there are firearms in the home
Making time for such conversations during routine care, including well-child visits
Paying special attention to warning signs of suicide and depression
Having frank conversations with parents about curious toddlers
“The safest home is a home without a firearm. If that’s not possible, the firearm should be stored in a locked cabinet with the ammunition stored separately,” she says. “Toddlers are especially curious and they actively explore their environment. An unsecured firearm can be a tragic accident waiting to happen with curious young children in the home. And if teenagers happen upon the weapon, it could be used in a homicide or suicide.”
In addition to empowering clinicians to have these conversations routinely, symposium speakers will emphasize empowering parents to ask other families: “Is there an unlocked gun in your house?”
“It’s no different than a parent of a child with a life-threatening sensitivity to peanuts asking if there are peanuts in any home that child may visit,” she adds. “As one of the leading causes of death among children and youth, unsecured firearms are even more dangerous than peanuts. And families should feel comfortable making informed decisions about whether their children will be safe as they play and socialize with friends.”
*** AAP National Conference and Exhibition presentation
Saturday, Oct. 26, 2:15 p.m. to 6:15 p.m. (ET)
“AAP NCE Section on Emergency Medicine/Section on Surgery/Section on Neurosurgery gun advocacy joint program”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/10/little-girl-reaching-for-gun.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2019-10-25 14:42:302024-11-27 09:43:46Empowering pediatricians to reduce preventable firearm injuries and deaths
Mihailo Kaplarevic, Ph.D., the newly minted Chief Research Information Officer at Children’s National Hospital and Bioinformatics Division Chief at Children’s National Research Institute, will provide computational support, advice, informational guidance, expertise in big data and data analyses for researchers and clinicians.
Kaplarevic’s new job is much like the role he played most recently at the National Heart, Lung and Blood Institute (NHLBI), assembling a team of researchers and scientists skilled in computing and statistical analyses to assist as in-house experts for other researchers and scientists.
NHLBI was the first institute within the National Institutes of Health (NIH) family to set up a scientific information office. During his tenure, a half-dozen other NIH institutions followed, setting up the same entity to help bridge the enormous gap between basic and clinical science and everything related to IT.
“There is a difference compared with traditional IT support at Children’s National – which will remain in place and still do the same sort of things they have been doing so far,” he says of The Bear Institute for Health Innovation. “The difference is this office has experience in research because every single one of us was a researcher at a certain point in our career: We are published. We applied for grants. We lived the life of a typical scientist. On top of that, we’re coming from the computational world. That helps us bridge the gaps between research and clinical worlds and IT.”
Ultimately, he aims to foster groundbreaking science by recognizing the potential to enhance research projects by bringing expertise acquired over his career and powerful computing tools to help teams achieve their goals in a less expensive and more efficient way.
“I have lived the life of a typical scientist. I know exactly how painful and frustrating it can be to want to do something quickly and efficiently but be slowed by technological barriers,” he adds.
As just one example, his office will design the high-performance computing cluster for the hospital to help teams extract more useful clinical and research data with fewer headaches.
Right now, the hospital has three independent clinical systems storing patient data; all serve a different purpose. (And there are also a couple of research information systems, also used for different purposes.) Since databases are his expertise, he will be involved in consolidating data resources, finding the best way to infuse the project with the bigger-picture mission – especially for translational science – and creating meaningful, actionable reports.
“It’s not only about running fewer queries,” he explains. “One needs to know how to design the right question. One needs to know how to design that question in a way that the systems could understand. And, once you get the data back, it’s a big set of things that you need to further filter and carefully shape. Only then will you get the essence that has clinical or scientific value. It’s a long process.”
As he was introduced during a Children’s National Research Institute faculty meeting in late-September 2019, Kaplarevic joked that his move away from pure computer science into a health care and clinical research domain was triggered by his parents: “When my mom would introduce me, she would say ‘My son is a doctor, but not the kind of doctor who helps other people.’ ”
Some of that know-how will play out by applying tools and methodology to analyze big data to pluck out the wheat (useful data) from the chaff in an efficient and useful way. On projects that involve leveraging cloud computing for storing massive amounts of data, it could entail analyzing the data wisely to reduce its size when it comes back from the cloud – when the real storage costs come in. “You can save a lot of money by being smart about how you analyze data,” he says.
While he expects his first few months will be spent getting the lay of the land, understanding research project portfolios, key principal investigators and the pediatric hospital’s biggest users in the computational domain, he has ambitious longer-term goals.
“Three years from now, I would like this institution to say that the researchers are feeling confident that their research is not affected by limitations related to computer science in general. I would like this place to become a very attractive environment for up-and-coming researchers as well as for established researchers because we are offering cutting-edge technological efficiencies; we are following the trends; we are a secure place; and we foster science in the best possible way by making computational services accessible, affordable and reliable.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/10/Mihailo-Kaplarevic.jpg400300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2019-10-04 13:58:382024-11-14 11:49:09Extracting actionable research data faster, with fewer hassles