

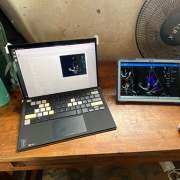
In December of 2024, a team that included experts from Children’s National Hospital traveled to Uganda to continue work on a pilot program applying artificial intelligence (AI) to the diagnosis of rheumatic heart disease (RHD). Ugandan health care providers have been trained and equipped to acquire echocardiograms for their patients but lack expertise in consistently being able to diagnose RHD by detecting leaky heart valves. The team created a tool that uses AI to predict RHD by identifying leaky heart valves on handheld ultrasound devices, then prompts a referral for a full echocardiogram.
The goal is to find ways to help people in Uganda diagnose RHD early, before a patient is in need of surgery, and initiate antibiotics so their heart can return to normal. The team of researchers, including fellow Kelsey Brown, MD, helped to implement additional steps toward this goal in December. According to Dr. Brown, the results were excellent. After four days of seeing patients, over 450 people were screened. The AI tool has an 86% accuracy rating. After returning from Uganda, the research team plans to work on the AI tool and further improve its accuracy rating. Eventually, the vision is that this tool can roll out on a larger scale for more places around the world to access it.
Craig Sable, MD, Marius Linguraru, DPhil, MA, MSc, and Pooneh Roshanitabrizi, PhD, from our Sheikh Zayed Institute, who developed the AI algorithms, worked in partnership with the Rheumatic Heart Disease Research Collaborative (RRCU) in Uganda. This trip was also made possible thanks to a grant funded through the Children’s National Global Health Initiative. Special thank you to our AI partner, US2.AI, who made the deployment of the AI models onto a tablet that provided real-time results, possible.

Our Global Health Initiative launched in 2016 with the goal of eliminating pediatric health disparities around the world. We aim to address the most pressing pediatric health issues through better care for medically underserved populations. This leadership helps us achieve our mission of caring for all children. A broad range of education and research projects improves health outcomes. They also offer enriching opportunities for experienced faculty and emerging leaders to advance clinical excellence.

Dr. Craig Sable and team train partners in Uganda.
Craig Sable, M.D., interim chief of Cardiology, improves care for young people with rheumatic heart disease (RHD) in Uganda. Donors, including the Karp Family Foundation, Huron Philanthropies, Zachary Blumenfeld Fund and the Wood family, make this possible. RHD affects 50 million people, mostly children, worldwide. It claims 400,000 lives each year.
Dr. Sable and Ugandan partners completed important research showing that early RHD detection, coupled with monthly penicillin treatment, can protect the heart. They are working on practical solutions, such as a new portable device with artificial intelligence (AI) that can easily screen for RHD.
In 2023, Dr. Sable led two missions in Uganda where he and his team did surgeries and special tests for 18 children with RHD. They also taught local doctors new skills to help more kids on their own.
Each year our Craniofacial & Pediatric Plastic Surgery team, under the leadership of Johnston Family Professor of Pediatric Plastic Surgery and Chief of Pediatric Plastic Surgery Gary Rogers, M.D., J.D., LL.M., M.B.A., M.P.H., provides opportunities for fellows to participate in surgical missions.
In 2024, Perry Bradford, M.D., traveled to the Moi Teaching Hospital in Eldoret, Kenya where she provided patients with burn, pressure wound and cleft reconstruction. She built community connections with the local plastic surgeons and educated registrars and medical students. “This gave me firsthand experience working in a community with limited resources and forced me to be more creative,” Dr. Bradford says. “The experience inspired me to examine what it means to have consistent access to advanced tools and equipment.”
In 2022, a group traveled to Nepal to provide care. Some patients arrived after days of travel by yak or buffalo. One child with a burn injury recovered use of her hand. The team educated local providers to deliver life-changing treatments unavailable in Nepal.

Dr. Tesfaye Zelleke, left, and team in Ethopia.
Neurologist Tesfaye Zelleke, M.D., and partners in Ethiopia are seeking to improve the lives of children with epilepsy. The BAND Foundation provides support. Ethiopia has a population of about 120 million yet only a handful of pediatric neurologists.
Dr. Zelleke’s team trained nonspecialist providers to diagnose and treat children in the primary care setting. They also launched a mobile epilepsy clinic to provide community care and build the capacity of local clinicians. In collaboration with advocacy groups, the team educates the public about epilepsy with a goal of reducing stigma.
In 2023, our Division of Colorectal & Pelvic Reconstruction shared its expertise with clinicians at Oslo University Hospital, Rikshospitalet, in Norway. This effort was a key first step in Oslo becoming the first dedicated colorectal center in Scandinavia.
Marc Levitt, M.D., and team members performed complex surgeries otherwise unavailable for waiting patients. They led an academic conference. They held clinics to educate nurses, reviewed patient records and made care recommendations. Specialized care enabled a young patient with significant bowel difficulties to recover function and lead a normal life.
The team will travel to South Africa, the Czech Republic and Spain in 2024. Donors, including The Dune Road Foundation and Deanna and Howard Bayless, make this work possible.
AI can be a valuable tool for diagnosing genetic conditions. It detects unique facial patterns that clinicians without genetics training can miss. However, existing facial analysis software struggles in nonwhite populations.
A team led by Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor of Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation, is working to improve the newborn diagnosis rate worldwide. They are testing smartphone software in the Democratic Republic of Congo. Diverse newborn data improves AI’s ability to detect a variety of genetic conditions in more children. Early detection, diagnosis and informed care lead to better health outcomes.

Jennifer Carver and Dr. Marva Moxey-Mims, center, with staff at Bustamante Children’s Hospital.
Marva Moxey-Mims, M.D., chief of Nephrology, is bringing care to children with kidney disease in Jamaica, with a goal of improving health equity. An International Pediatric Nephrology Association grant helped make it possible.
On a recent trip, Dr. Moxey-Mims and a small team — including Jennifer Carver, RN, CNN, lead peritoneal dialysis nurse at Children’s National, and three pediatric nephrologists from Jamaica — trained nearly 30 nurses from Jamaican hospitals. Nurses received hands-on dialysis education to improve their clinical skills. The team also worked to educate the community in disease awareness and prevention.
Read more stories like this one in the latest issue of Believe magazine.

In the complex world of pediatric diseases, researchers need access to data to develop clinical trials and the participation of vulnerable patients to develop new devices and therapies. Both are in short supply, given that most children are born healthy, and most severe pediatric diseases are rare.
That creates a dilemma: how do researchers build a foundation to advance new treatments? Enter artificial intelligence (AI).
“AI is the equalizer: accelerated intelligence for sick kids. No other advance on the horizon holds more promise for improving equity and access to pediatric healthcare when diseases are rare and resources are limited,” says Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor in Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI). “AI will shrink the distance between patient and provider, allowing our physicians and scientists to provide targeted healthcare for children more efficiently. The possibilities are endless.”
By pioneering AI innovation programs at Children’s National Hospital, Dr. Linguraru and the AI experts he leads are ensuring patients and families benefit from a coming wave of technological advances. The team is teaching AI to interpret complex data that could otherwise overwhelm clinicians. Their work will create systems to identify at-risk patients, forecast disease and treatment patterns, and support complex clinical decisions to optimize patient care and hospital resources. Already, the AI team at SZI has developed data-driven tools touching nearly every corner of the hospital:
Looking ahead, the Children’s National AI team is pursuing a wide range of advances in clinical care. To support patients treated at multiple clinics, they are developing systems to harmonize images from different scanners and protocols, such as MRI machines made by different manufacturers. Similar work is underway to analyze pathology samples from different institutions consistently.
Automation is also making care more efficient. For example, using data from 1 million chest X-rays, the team is collaborating with NVIDIA to develop a conversational digital assistant that will allow physicians to think through 14 possible diagnoses.
Dr. Linguraru says he and his colleagues are galvanized by the jarring statistic that one in three children with a rare disease dies before age 5. While well-implemented AI initiatives can change outcomes, he says the work must be done thoughtfully.
“In the future, patients will be evaluated by human clinicians and machines with extraordinary powers to diagnose illness and determine treatments,” Dr. Linguraru said. “Our team at Children’s National is leading conversations about the future of pediatric healthcare with a focus on safety, resource allocation and basic equity.”
Artificial intelligence (AI) has the potential to detect rheumatic heart disease (RHD) with the same accuracy as a cardiologist, according to new research demonstrating how sophisticated deep learning technology can be applied to this disease of inequity. The work could prevent hundreds of thousands of unnecessary deaths around the world annually.
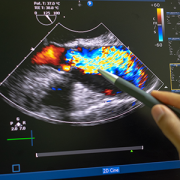
Developed at Children’s National Hospital and detailed in the latest edition of the Journal of the American Heart Association, the new AI system combines the power of novel ultrasound probes with portable electronic devices installed with algorithms capable of diagnosing RHD on echocardiogram. Distributing these devices could allow healthcare workers, without specialized medical degrees, to carry technology that could detect RHD in regions where it remains endemic.
RHD is caused by the body’s reaction to repeated Strep A bacterial infections and can cause permanent heart damage. If detected early, the condition is treatable with penicillin, a widely available antibiotic. In the United States and other high-income nations, RHD has been almost entirely eradicated. However, in low- and middle-income countries, it impacts the lives of 40 million people, causing nearly 400,000 deaths a year.
“This technology has the potential to extend the reach of a cardiologist to anywhere in the world,” said Kelsey Brown, M.D., a cardiology fellow at Children’s National and co-lead author on the manuscript with Staff Scientist Pooneh Roshanitabrizi, Ph.D. “In one minute, anyone trained to use our system can screen a child to find out if their heart is demonstrating signs of RHD. This will lead them to more specialized care and a simple antibiotic to prevent this degenerative disease from critically damaging their hearts.”

The new AI system combines the power of novel ultrasound probes with portable electronic devices installed with algorithms capable of diagnosing RHD on echocardiogram.
Millions of citizens in impoverished countries have limited access to specialized care. Yet the gold standard for diagnosing RHD requires a highly trained cardiologist to read an echocardiogram — a non-invasive and widely distributed ultrasound imaging technology. Without access to a cardiologist, the condition may remain undetected and lead to complications, including advanced cardiac disease and even death.
According to the new research, the AI algorithm developed at Children’s National identified mitral regurgitation in up to 90% of children with RHD. This tell-tale sign of the disease causes the mitral valve flaps to close improperly, leading to backward blood flow in the heart.
Beginning in March, Craig Sable, M.D., interim division chief of Cardiology, and his partners on the project will implement a pilot program in Uganda incorporating AI into the echo screening process of children being checked for RHD. The team believes that a handheld ultrasound probe, a tablet and a laptop — installed with the sophisticated, new algorithm — could make all the difference in diagnosing these children early enough to change outcomes.
“One of the most effective ways to prevent rheumatic heart disease is to find the patients that are affected in the very early stages, give them monthly penicillin for pennies a day and prevent them from becoming one of the 400,000 people a year who die from this disease,” Dr. Sable said. “Once this technology is built and distributed at a scale to address the need, we are optimistic that it holds great promise to bring highly accurate care to economically disadvantaged countries and help eradicate RHD around the world.”
To devise the best approach, two Children’s National experts in AI — Dr. Roshanitabrizi and Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor in Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation — tested a variety of modalities in machine learning, which mimics human intelligence, and deep learning, which goes beyond the human capacity to learn. They combined the power of both approaches to optimize the novel algorithm, which is trained to interpret ultrasound images of the heart to detect RHD.
Already, the AI algorithm has analyzed 39 features of hearts with RHD that cardiologists cannot detect or measure with the naked eye. For example, cardiologists know that the heart’s size matters when diagnosing RHD. Current guidelines lay out diagnostic criteria using two weight categories — above or below 66 pounds — as a surrogate measure for the heart’s size. Yet the size of a child’s heart can vary widely in those two groupings.
“Our algorithm can see and make adjustments for the heart’s size as a continuously fluid variable,” Dr. Roshanitabrizi said. “In the hands of healthcare workers, we expect the technology to amplify human capabilities to make calculations far more quickly and precisely than the human eye and brain, saving countless lives.”
Among other challenges, the team had to design new ways to teach the AI to handle the inherent clinical differences found in ultrasound images, along with the complexities of evaluating color Doppler echocardiograms, which historically have required specialized human skill to evaluate.
“There is a true art to interpreting this kind of information, but we now know how to teach a machine to learn faster and possibly better than the human eye and brain,” Dr. Linguraru said. “Although we have been using this diagnostic and treatment approach since World War II, we haven’t been able to share this competency globally with low- and middle-income countries, where there are far fewer cardiologists. With the power of AI, we expect that we can, which will improve equity in medicine around the world.”


Although entirely preventable, RHD, a disease of poverty and social disadvantage resulting in high morbidity and mortality, remains an ever-present burden in low- and middle-income countries, as well as rural, remote, marginalized and disenfranchised populations within high-income countries.
A rheumatic heart disease (RHD) work group convened by the National Heart, Lung, and Blood Institute (NHLBI) concludes that any priority intervention strategies to slow or stop late complications of RHD need to consider local contexts and should be integrated into health systems to meet the affected community’s needs in a sustainable way.
The group outlined priorities based on current available evidence to support the development and implementation of accessible, affordable and sustainable interventions in low-resource settings to manage RHD and its related complications.
Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital, served as a senior author on the recommendations, based on the work group findings.
Although entirely preventable, RHD, a disease of poverty and social disadvantage resulting in high morbidity and mortality, remains an ever-present burden in low- and middle-income countries, as well as rural, remote, marginalized and disenfranchised populations within high-income countries.
The NHLBI workshop sought to support RHD eradication efforts worldwide by:
Each work group was assigned to review existing guidelines and research for different stages of the disease’s progression, which is now being published together as a set of five companion articles to raise the prioritization of RHD research and funding.
Due to the high prevalence of RHD in low- and middle-income countries, Dr. Sable’s work group focused on gaining a better understanding of the needs in the field from the five perspectives: people living with RHD, the community, healthcare providers, health systems and policymakers.
They identified several priorities and strategies, and they stressed that any interventional strategy, now or in the future, must be culturally safe and community-driven to ensure the creation of a locally and culturally relevant, sustainable continuum of care for people from historically marginalized populations.
The authors emphasize that that over 300,000 deaths per year are the result of inadequate, underfunded and poorly integrated care. “Global vision and leadership to enact and implement available policies are needed to close large research gaps in all aspects at patient, health system and policy levels. Robust research and development are urgently needed to improve comprehensive tertiary care and ensure implementation of evidence-based interventions, while developing new innovations, technologies and interventions.”
You can read all the working group manuscripts, including this one: Tertiary Prevention and Treatment of Rheumatic Heart Disease: A National Heart, Lung, and Blood Institute Working Group Summary, in BMJ Global Health.
Learn more about the challenges of rheumatic heart disease in sub-Saharan Africa and other developing parts of the world through the Rheumatic Heart Disease microdocumentary series:
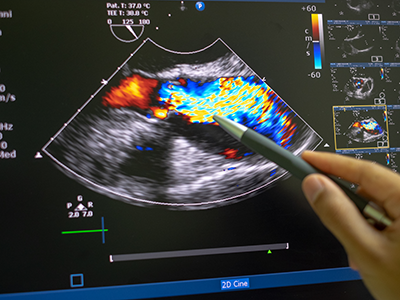
Researchers at Children’s National Hospital have created a new artificial intelligence (AI) algorithm that promises to be as successful at detecting early signs of rheumatic heart disease (RHD) in color Doppler echocardiography clips as expert clinicians.
Researchers at Children’s National Hospital have created a new artificial intelligence (AI) algorithm that promises to be as successful at detecting early signs of rheumatic heart disease (RHD) in color Doppler echocardiography clips as expert clinicians. Even better, this novel model diagnoses this deadly heart condition from echocardiography images of varying quality — including from low-resource settings — a huge challenge that has delayed efforts to automate RHD diagnosis for children in these areas.
Current estimates are that 40.5 million people worldwide live with rheumatic heart disease, and that it kills 306,000 people every year. Most of those affected are children, adolescents and young adults under age 25.
Though widely eradicated in nations such as the United States, rheumatic fever remains prevalent in developing countries, including those in sub-Saharan Africa. Recent studies have shown that, if detected soon enough, a regular dose of penicillin may slow the development and damage caused by RHD. But it has to be detected.
Diagnosing RHD requires an ultrasound image of the heart, known as an echocardiogram. However, ultrasound in general is very variable as an imaging modality. It is full of texture and noise, making it one of the most challenging to interpret visually. Specialists undergo significant training to read them correctly. However, in areas where RHD is rampant, people who can successfully read these images are few and far between. Making matters worse, the devices used in these low resource settings have their own levels of varying quality, especially when compared to what is available in a well-resourced hospital elsewhere.
The research team hypothesized that a novel, automated deep learning-based method might detect successfully diagnose RHD, which would allow for more diagnoses in areas where specialists are limited. However, to date, machine learning has struggled the same way the human eye does with noisy ultrasound images.
Using approaches that led to successful objective digital biometric analysis software for non-invasive screening of genetic disease, researchers at the Sheikh Zayed Institute for Pediatric Surgical Innovation, including medical imaging scientist Pooneh Roshanitabrizi, Ph.D., and Marius Linguraru, D.Phil., M.A., M.Sc., principal investigator, partnered with clinicians from Children’s National Hospital, including Craig Sable, M.D., associate chief of Cardiology and director of Echocardiography, and cardiology fellow Kelsey Brown, M.D., who are heavily involved in efforts to research, improve treatments and ultimately eliminate the deadly impacts of RHD in children. The collaborators also included cardiac surgeons from the Uganda Heart Institute and cardiologists from Cincinnati Children’s Hospital Medical Center.
Dr. Linguraru’s team of AI and imaging scientists spent hours working with cardiologists, including Dr. Sable, to truly understand how they approach and assess RHD from echocardiograms. Building the tool based on that knowledge is why this tool stands apart from other efforts to use machine-learning for this purpose. Orienting the approach to the clinical steps of diagnosis is what led to the very first deep learning algorithm that diagnoses mild RHD with similar success to the specialists themselves. After the platform was built, 2,136 echocardiograms from 591 children treated at the Uganda Heart Institute fed the learning algorithm.
The team will continue to collect data points based on clinical imaging data to refine and validate the tool. Ultimately, researchers will look for a way that the algorithm can work directly with ultrasound/echocardiogram machines. For example, the program might be run through an app that sits on top of an ultrasound device and works on the same platform to communicate directly with it, right in the clinic. By putting the two technologies together, care providers on the ground will be able to diagnose mild cases and prescribe prophylactic treatments like penicillin in one visit.
The first outcomes from the program were showcased in a presentation by Dr. Roshanitabrizi at one of the biggest and most prestigious medical imaging and AI computing meetings — the 25th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI).


“We know from previous studies that though it is not always well-documented, sub-Saharan Africa continues to have some of the highest numbers of people with rheumatic heart disease and the highest numbers of people dying from it,” said Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital and co-senior author of the study. “This study is the first large-scale clinical trial to show that early detection coupled with prophylactic treatment of penicillin is feasible and can prevent rheumatic heart disease from progressing and causing further damage to a child’s heart.”
Penicillin, a widely available and affordable antibiotic, may be one key to turning the tide on the deadly impacts of rheumatic heart disease (RHD) for children in developing nations. This according to the new findings of a large-scale, randomized controlled trial completed in Uganda and published in the New England Journal of Medicine.
The most devastating feature of RHD is severe heart valve damage that is caused by rheumatic fever — a condition that results from the body’s immune system trying to fight poorly treated, repeat infections from streptococcus bacteria, also known as strep throat. Though widely eradicated in nations such as the United States due to the swift detection and treatment of strep throat, rheumatic fever remains prevalent in developing countries including those in sub-Saharan Africa. Current estimates are that 40.5 million people worldwide live with rheumatic heart disease, and that it kills 306,000 people every year. Most of those affected are children, adolescents and young adults under age 25.
“We know from previous studies that though it is not always well-documented, sub-Saharan Africa continues to have some of the highest numbers of people with rheumatic heart disease and the highest numbers of people dying from it,” said Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital and co-senior author of the study. “This study is the first large-scale clinical trial to show that early detection coupled with prophylactic treatment of penicillin is feasible and can prevent rheumatic heart disease from progressing and causing further damage to a child’s heart.”
The study was led by an international panel of pediatric cardiac experts from institutions including Children’s National, Cincinnati Children’s Medical Center, the Uganda Heart Institute and Murdoch Children’s Research Institute in Melbourne, Australia.
“Our study found a cheap and easily available penicillin can prevent progression of latent rheumatic heart disease into more severe, irreversible valve damage that is commonly seen in our hospitals with little or no access to valve surgery,” said co-lead author Emmy Okello, M.D., chief of Cardiology at the Uganda Heart Institute.
To Andrea Beaton, M.D., associate professor of Cardiology at Cincinnati Children’s and co-lead author, this is the first contemporary randomized controlled trial in rheumatic heart disease. “The results are incredibly important on their own, but also demonstrate that high-quality clinical trials are feasible to address this neglected cardiovascular disease,” she said.
Beaton et al. named the trial Gwoko Adunu pa Lutino (GOAL), which means “protect the heart of a child.” The study enrolled 818 Ugandan children and adolescents ages 5 to 17 years old who were diagnosed with latent rheumatic heart disease to see if an injection of penicillin was effective at preventing their heart condition from worsening.
“There are many challenges with recruitment and retention of trial participants in areas like our study region in Uganda,” said Dr. Sable. “But it is critical to work together and overcome barriers, because we must study these treatments in the people most affected by the condition to understand how they, and others like them, may benefit from the findings.”
Of the 799 participants who completed the trial, the group receiving a prophylactic injection of penicillin (399 volunteers) had three participants show evidence of worsened rheumatic heart disease on repeat echocardiogram after two years. In contrast, 33 of the 400 volunteers in the control group, who received no treatment, showed similar progression on echocardiogram results.
Professor Andrew Steer, who is theme director of Infection and Immunity at Murdoch Children’s Research Institute in Melbourne and who served as senior author of the study, said screening for latent rheumatic heart disease was critical to stop progression because heart valve damage was largely untreatable. “Most patients are diagnosed when the disease is advanced and complications have already developed. If patients can be identified early, there is an opportunity for intervention and improved health outcomes.”
The results were shared in a special presentation at the American Heart Association’s Scientific Sessions on the same day that the findings were published in the New England Journal of Medicine.
The trial was supported by the Thrasher Pediatric Research Fund, Gift of Life International, Children’s National Hospital Foundation: Zachary Blumenfeld Fund, Children’s National Hospital Race for Every Child: Team Jocelyn, the Elias/Ginsburg Family, Wiley-Rein LLP, Phillips Foundation, AT&T Foundation, Heart Healers International, the Karp Family Foundation, Huron Philanthropies and the Cincinnati Children’s Hospital Heart Institute Research Core.
Learn more about the challenges of rheumatic heart disease in sub-Saharan Africa and other developing parts of the world through the Rheumatic Heart Disease microdocumentary series:


Despite low numbers of documented acute rheumatic fever cases in sub-Saharan Africa, the region continues to show some of the highest numbers of people with, and dying from, rheumatic heart disease, the serious heart damage caused by repeat instances of rheumatic fever.
Despite low numbers of documented acute rheumatic fever cases in sub-Saharan Africa, the region continues to show some of the highest numbers of people with, and dying from, rheumatic heart disease, the serious heart damage caused by repeat instances of rheumatic fever. A population-based study in the Lancet Global Health collected evidence of acute rheumatic fever in two areas of Uganda, providing the first quantifiable evidence in decades that the disease continues to take a deadly toll on the region’s people.
“These findings matter. Access to life-saving heart surgery is only available to a very small fraction of the hundreds of thousands of patients in Africa who have irreversible heart damage from rheumatic heart disease,” says Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital and one of the senior authors of the study. “It’s time to focus upstream on capturing these conditions sooner, even in low-resource settings, so we can implement life-sustaining and cost-saving preventive treatments that can prevent further heart damage.”
The authors, who hail from Uganda and several institutions around the United States, including Children’s National and Cincinnati Children’s Hospital Medical Center, note this is the first study to use an active case-finding strategy for diagnosing acute rheumatic fever. They also note that raising awareness in the community and among its healthcare workers while also finding new ways to overcome some of the diagnostic challenges in these low-resource settings greatly improved diagnosis and treatment of the condition.
The study also described clinical characteristics of children ages 5 to 14 presenting with both definitive and possible acute rheumatic fever, providing further clinical data points to help healthcare workers in these communities differentiate between this common infection and some of the other frequently diagnosed conditions in the region.
“With this study, we can now confidently dismiss the myth that acute rheumatic fever is rare in Africa,” the authors write. “It exists at elevated rates in low-resource settings such as Uganda, even though routine diagnosis remains uncommon. While these incidence data have likely underestimated the cases of acute rheumatic fever in two districts in Uganda, they show that opportunity exists to improve community sensitization and healthcare worker training to increase awareness of acute rheumatic fever. Ultimately this leads to diagnosing more children with the condition before they develop rheumatic heart disease, so that they can be offered secondary prophylaxis with penicillin.”
Children with suspected acute rheumatic fever participated in this population-based study. Data was collected over 12 months in Lira district (January 2018 to December 2018) and over nine months (June 2019 to February 2020) in Mbarara district.
Follow-up of children diagnosed in this study will provide more data on the outcomes of acute rheumatic fever, including a better understanding of the risk for a child to develop rheumatic heart disease.
This work was funded by the American Heart Association Children’s Strategically Focused Research Network Grant #17SFRN33670607 and by DEL‐15‐011 to THRiVE‐2 and General Electric.
Learn more about the challenges of rheumatic heart disease in sub-Saharan Africa and other developing parts of the world through the Rheumatic Heart Disease microdocumentary series:


Sub-Saharan Africa has only 0.19 pediatric cardiac surgeons per million children — nowhere near enough surgeons to care for all the pediatric congenital heart disease and acquired heart disease present in the people who live there.
A literature review in the journal Current Opinion in Cardiology draws further attention to the pressing needs for better pediatric cardiac care in regions of the world where the population continues to grow, but the development of specialty care for children continues to lag. The article focuses specifically on sub-Saharan Africa.
“If 40% of live births occur in Africa by 2050 as the projections suggest, congenital heart disease may well become the most important contributor to infant mortality rate in sub-Saharan Africa in the next three decades,” stated the authors, including Annette Ansong, M.D., who recently joined Children’s National Hospital as medical director of outpatient cardiology.
As highlighted previously by other authors within the Global Health Initiative at Children’s National and through the work of the American Heart Association, the region’s needs are already significant in tackling the impacts of existing congenital heart disease and rheumatic heart disease. Rheumatic heart disease is a devastating long-term outcome of rheumatic fever caused by untreated streptococcus infections.

“If 40% of live births occur in Africa by 2050 as the projections suggest, congenital heart disease may well become the most important contributor to infant mortality rate in sub-Saharan Africa in the next three decades,” stated the authors, including Annette Ansong, M.D., who recently joined Children’s National Hospital as medical director of outpatient cardiology.
Dr. Ansong and colleagues reiterate the point that today, “whereas one cardiac center caters to approximately 120,000 people in North America, 33 million people in sub-Saharan Africa must depend on one center for care.” They also note that this region of Africa has only 0.19 pediatric cardiac surgeons per million children compared with more than 58 times as many in North America.
Changing the trajectory of pediatric cardiac care in sub-Saharan Africa will take motivation on several fronts, the authors write. Dedication to early detection and intervention (medical or surgical), an emphasis on building an in-country pipeline of human resources and skills’ sets are needed to tackle the increasing numbers of children requiring this specialty care. Political will and better financial resources can also support the training and development of centers that specialize in these capabilities.

Dr. Craig Sable and pediatric cardiology colleagues led the creation of a scientific statement and advocacy statement focused on eradicating RHD.
A pair of articles appearing in the American Heart Association’s (AHA) journal Circulation lays out a call to action for advocacy and scientific priorities crucial to the global eradication of rheumatic heart disease (RHD).
Cardiologists from Children’s National Hospital, and others who completed their pediatric cardiology fellowships at Children’s National before moving on to careers at other institutions, have been active proponents and advocates for these efforts for many years and led key research and clinical care efforts related to RHD in other countries of the world.
These cardiologists, including the associate chief of cardiology at Children’s National, Craig Sable, M.D., who previously served as chair of the AHA Council on Lifelong Congenital Heart Disease and Heart Health in the Young, also helped lead the creation of these new published statements.
Contemporary diagnosis and management of rheumatic heart disease: Implications for closing the gap
This clinical and research statement “seeks to examine the current state of-the-art recommendations and to identify gaps in diagnosis and treatment globally that can inform strategies for reducing disease burden.”
Key recommendations and related challenges were mapped out, including:
The recommendations made in the scientific statement form the foundation for the advocacy companion document.
The AHA’s call to action for reducing the global burden of rheumatic heart disease: a policy statement from the AHA
The advocacy statement outlines five key areas of support:
The authors write, “In bolstering the efforts of the American Heart Association to combat RHD, we hope to inspire others to collaborate, communicate and contribute.”
Speaking of the two statements as a whole, the authors of the scientific statement conclude that, “Ultimately, the combination of expanded treatment options, research and advocacy built on existing knowledge and science provides the best opportunity to address the burden of rheumatic heart disease.”
Read more about Children’s National Heart Institute’s research, education and clinical care in rheumatic heart disease.
Craig Sable, M.D., Associate Chief of the Division of Cardiology and Director of Echocardiography at Children’s National Health System, is working with hundreds of doctors to create a scalable solution to reduce the global burden of rheumatic heart disease (RHD). Dr. Sable received a lifetime achievement award — the 2018 Cardiovascular Disease in the Young (CVDY) Meritorious Achievement Award — from the American Heart Association for his work in Uganda.


Patients and staff at the Uganda Heart Institute for RHD-related heart surgeries in Uganda, March 2020. These patients were originally scheduled as part of the cancelled medical mission, but UHI cardiovascular surgeon successfully managed these cases without the support of the mission doctors from the U.S.
In early March as countries around the globe began to wrestle with how best to tackle the spread of COVID-19, a group of doctors, nurses, researchers and other medical staff from Children’s National Hospital were wrestling with a distinct set of challenges: What to do about the 10 Ugandan children and adults who were currently scheduled for lifesaving heart surgery (and the countless others who would benefit from the continued training of the local heart surgery team) to correct complications of rheumatic heart disease (RHD) during an impending medical mission in the country.
Rheumatic heart disease impacts over 39 million people globally and causes nearly 300,000 deaths per year. RHD is the result of frequent, untreated streptococcal throat infections in childhood that ultimately cause the body’s immune system to repeatedly damage heart valves. It is completely preventable, yet the majority of the world’s children still live in impoverished and overcrowded conditions that predispose them to RHD. Most patients present with advanced valvular heart disease. For example, in Uganda, an RHD registry includes over 600 children with clinical RHD, of which nearly 40% die within four years and the median survival time from enrollment in the registry is only nine months. For these patients, heart surgery is the only viable solution for long-term survival and normal quality of life.

Patricia: 9-year-old from Gulu (northern Uganda), had mitral valve replacement and was doing well on a recent follow-up visit at her home.
The scheduled trip from Washington was part of a nearly 20-year partnership** between doctors, nurses, researchers and other medical staff in the United States, including Craig Sable, M.D., associate chief of cardiology, and and Pranava Sinha, M.D.,pediatric cardiovascular surgeon, at Children’s National Hospital in Washington, D.C., and the Uganda Heart Institute in Kampala, Uganda. The partnership aims to tackle RHD head-on. It provides surgical skill transfer, allows for treatment of more complex patients, and increases sustainable surgical capacity for Uganda’s RHD patients over time. As a result, over the last 15 years more than 1,000 children have received lifesaving heart surgery in Uganda, with the Uganda Heart Institute (UHI) performing one to two heart valve surgeries every two weeks over the last few years.

Jackline: 12-year-old from Gulu, had mitral valve repair and aortic valve replacement. Jackline and Patricia were diagnosed through one of our research programs and benefit from our novel telehealth program, which helps connect patients from remote parts of Uganda to specialists at UHI.
COVID-19 was changing the current plan, however. Travel between countries was limited, and the team from the U.S. wouldn’t have been permitted to leave the U.S. and return according to schedule. The trip, and the support teams who were scheduled to arrive to help with the surgeries, were cancelled. The U.S. team members who had already arrived in Uganda were sent home after helping their UHI colleagues set up and prepare for the surgeries as much as possible. Knowing that patients and families were counting on the surgery mission to go forward after waiting for months or years to have surgery for heart valve disease, UHI decided not to cancel the majority of the surgeries. Instead, for the first time, they planned and successfully completed five valve-related cases in a single week – several of them quite complex. The cardiologists and cardiac surgeons from Children’s National who were supposed to be in-country for these procedures were forced to limit their in person assistance to the set-up activities the week prior to surgery and telehealth consult during the procedures.
“It was hard not to be able to stay and work with the UHI team to help these families,” says Dr. Sable. “But we are so proud of the UHI team for meeting this challenge on their own. We knew they had the skills to perform at this volume and complexity. It’s a proud moment to see the team accomplish this major milestone, and to see the patients they cared for thrive.”
The patients are the most important outcome: The five who had successful open-heart surgery are all doing well, either on their way to recovery or already discharged to their communities, where they will, for the first time in memory, be able to play, exercise and go to school or work.
Longer term, this success demonstrates the UHI medical team’s ability to manage greater surgical capacity even when surgical missions from the U.S. resume. The partnership’s goal is to complete at least 1,000 annual operations (both pediatric and adult), with the majority being performed by the local team. Having this capacity available will mean the difference between life and death for many children and adults who have RHD in Uganda and the surrounding countries.
**This work is supported by the Edwards Life Sciences/Thoracic Surgery Foundation, the Emirates Airline Foundation, Samaritan’s Purse Children’s Heart Project and Gift of Life International.

Craig Sable, M.D., associate chief of the division of cardiology and director of echocardiography at Children’s National Health System, earned a lifetime achievement award, formally known as the 2018 Cardiovascular Disease in the Young (CVDY) Meritorious Achievement Award, on Nov. 10 at the American Heart Association’s Scientific Sessions 2018.
The CVDY Council bestows the prestigious award to individuals making a significant impact in the field of cardiovascular disease in the young. The CVDY Council supports the mission to improve the health of children and adults with congenital heart disease and acquired heart disease during childhood through research, education, prevention and advocacy.
Dr. Sable is recognized for his entire body of research, education and advocacy focused on congenital and acquired heart disease, but especially for his rheumatic heart disease (RHD) research in Uganda.
Over the past 15 years, Dr. Sable has brought more than 100 doctors and medical staff to Kampala, the capital and largest city in Uganda, partnering with more than 100 local doctors and clinicians to develop a template for a sustainable infrastructure to diagnose, treat and prevent both RHD and congenital heart disease.
RHD is a result of damage to the heart valves after acute rheumatic fever (ARF). The process starts with a sore throat from streptococcal infection, which many children in the United States treat with antibiotics.
“For patients who develop strep throat, their body’s reaction to the strep throat, in addition to resolving its primary symptoms, can result in attacking the heart,” says Dr. Sable. “The initial damage is called acute rheumatic fever. In many cases this disease is self-limited, but if undetected, over years, it can lead to long-term heart valve damage called rheumatic heart disease. Unfortunately, once severe RHD develops the only treatment is open-heart surgery.”
In 2017, Sable and the researchers published a study in the New England Journal of Medicine about the global burden of RHD, which is often referred to as a disease of poverty.
RHD is observed more frequently in low- and middle-income countries as well as in marginalized communities in high-income countries. RHD has declined on a global scale, but it remains the most significant cause of morbidity and mortality from heart disease in children and young adults throughout the world.
In 2017 there were 39.4 million causes of RHD, which resulted in 285,000 deaths and 9.4 million disability-adjusted life-years.
In 2018 the World Health Organization issued a referendum recognizing rheumatic heart disease as an important disease that member states and ministries of health need to prioritize in their public health efforts.
The common denominator that drives Dr. Sable and the global researchers, many of whom have received grants from the American Heart Association to study RHD, is the impact that creating a scalable solution, such as widespread adoption of vaccines, can have on entire communities.
“The cost of an open-heart surgery in Uganda is $5,000 to $10,000, while treatment for a child with penicillin for one year costs less than $1,” says Dr. Sable. “Investment in prevention strategies holds the best promise on a large scale to eradicate rheumatic heart disease.”
Sable and the team have screened more than 100,000 children and are conducting the first randomized controlled RHD trial, enrolling nearly 1,000 children, to examine the effectiveness of using penicillin to prevent progression of latent or subclinical heart disease, the earliest form of RHD.
During the Thanksgiving holiday weekend, Dr. Sable and a team of surgeons will fly back to Uganda to operate on children affected by RHD, while also advancing their research efforts to produce a scalable solution, exported on a global scale, to prevent RHD in its earliest stages.
Dr. Sable and colleagues from around the world partner on several grant-funded research projects. Over the next few years, the team hopes to answer several important questions, including: Does penicillin prevent the earliest form of RHD and can we develop a vaccine to prevent RHD?
To view the team’s previously-published research, visit Sable’s PubMed profile.
To learn about global health initiatives led by researchers at Children’s National, visit www.GHICN.org.

Rheumatic heart disease is caused by untreated throat infections from the streptococcal bacterium. The infections progress into acute rheumatic fever and eventually weaken the valves of the heart.
Rheumatic heart disease (RHD) is the most commonly acquired cardiovascular disease in children and young adults. The devastating condition, which was endemic in the United States before 1950, is now relatively rare in the developed world due to social and economic development and the introduction of penicillin. But, in the developing world RHD remains nearly as common as HIV.
Fortunately, RHD is a cumulative disease and opportunities exist for early intervention. To further explore the utility of early diagnosis and intervention, a research team headed by Children’s National Heart Institute cardiologist Andrea Beaton, M.D., conducted a prospective natural history study of children with latent RHD.
RHD is caused by untreated streptococcal throat infections that progress into acute rheumatic fever (ARF) and eventually weaken the valves of the heart. While initial episodes of ARF occur almost exclusively during childhood, RHD most commonly presents in adolescents and young adults. This latent period between ARF and clinically apparent RHD is an ideal opportunity for early intervention, and screening echocardiography (echo) has emerged as a potentially powerful tool for early detection of RHD.
In their study published in the journal Circulation in September 2017, Dr. Beaton and her colleagues examined echocardiograms from children with latent RHD who were enrolled in the Ugandan National RHD registry. The researchers also developed models to search for risk factors and compare progression-free survival between patients who did and did not receive penicillin.
The team reports that children with moderate-to-severe latent RHD discovered by echo screening have poor outcomes. Children with both borderline and mild definite RHD have better outcomes but remain at substantial risk of progression. The researchers also found that children who are diagnosed at a younger age, and the presence of morphological mitral valve features, generally lead to unfavorable outcomes.
The authors conclude that children with moderate to severe RHD at screening should be considered for treatment as clinically diagnosed RHD, and that children with borderline or mild definite RHD at screening should, at a minimum, be maintained in close clinical follow up.
“It is clear that children found to have the earliest forms of RHD, seen only by echo, are at substantial risk for progression of disease. This study urges us forward to see if we can intervene to stop this progression once children are identified,” says Dr. Beaton. “We are excited that our next project will be to do just that – a randomized clinical trial in Uganda to determine if penicillin can protect the hearts of children found to have latent RHD.”

A research team that included Children’s National Heart Institute experts Andrea Beaton, M.D., and Craig Sable, M.D., examined data on fatal and nonfatal Rheumatic Heart Disease for a 25 year period from 1990 through 2015 to determine the current global burden of RHD.
Rheumatic Heart Disease (RHD) is the most commonly acquired heart disease in young people under the age of 25. It’s caused by untreated streptococcal throat infections that progress into acute rheumatic fever and eventually weaken the valves of the heart. Fortunately, the devastating condition, which was endemic in the United States before 1950, is now relatively rare in the developed world due to social and economic development and the introduction of penicillin. But, as shown in a recent study published in the New England Journal of Medicine, in the developing world, RHD remains nearly as common as HIV.
As part of the 2015 Global Burden of Disease Study, a research team that included Children’s National Heart Institute experts Andrea Beaton, M.D., and Craig Sable, M.D., examined data on fatal and nonfatal RHD for a 25 year period from 1990 through 2015 to determine the current global burden of RHD. The group employed epidemiologic modeling techniques to estimate the global, regional and national prevalence of RHD, as well as death rates and disability-adjusted life years attributable to the disease.
“This study provides more detail than ever before about the global impact of RHD,” explains Dr. Sable. “It utilizes global burden of disease tools that are updated on an annual basis. These tools are considered highly reputable and allow for ongoing tracking and comparison to other diseases.”
The researchers found that overall, death rates from RHD have declined: there were 347,500 deaths from RHD in 1990 and 319,400 deaths in 2015, a decrease of 8 percent. From 1990 to 2015, the global age-standardized death rate from RHD also decreased from 9.2 to 4.8 per 100,000 — a change of 48 percent.
However, a closer look at the data shows that progress on RHD remains uneven. Although the health-related burden of RHD has declined in most countries over the 25-year period, the condition persists in some of the poorest regions in the world, with the highest estimated death rates in Central African Republic, Federated States of Micronesia, Fiji, India, Kiribati, Lesotho, Marshall Islands, Pakistan, Papua New Guinea, the Solomon Islands and Vanuatu. In several regions, mortality from RHD and the number of individuals living with RHD did not appreciably decline between 1990 and 2015. The researchers estimate that 10 out of every 1,000 people living in South Asia and central sub-Saharan Africa and 15 out of 1,000 people in Oceania were living with RHD in 2015.
“These data are critically important for increasing awareness and funding to reduce the global burden of rheumatic heart disease,” says Dr. Sable. “Dr. Beaton and I are proud to be part of a small team of global investigators leading this effort.”
Children’s National Health System was recently awarded a grant from the American Heart Association to launch a Rheumatic Heart Disease Center, with the goal of developing innovative strategies and economic incentives to improve the prevention and diagnosis of RHD in high-risk, financially disadvantaged countries and low-income communities across the United States. The program will use Children’s robust telemedicine infrastructure to connect co-collaborators around the world, as well as train the next generation of globally minded cardiovascular researchers.


Ten-year-old Angioletta was clinically diagnosed with rheumatic heart disease in 2014 (severe leakage of her mitral valve). She’s been medically managed at the clinic Children’s helps support and conducts research at in Gulu, and she is a very active participant in the support group led by Children’s National research assistant, Amy Scheel. Angioletta hasn’t had any major complications, but her only hope for long-term survival is to undergo open heart surgery to replace her abnormal valve. Experts are looking towards the research from the new Center to help prevent future generations of children like Angioletta from developing RHD.
Known as the ‘world’s forgotten disease,’ Rheumatic Heart Disease (RHD) is caused by untreated streptococcal throat infections that progress into acute rheumatic fever (ARF) and eventually weaken the valves of the heart. It is the most common cardiovascular disease in children and young adults globally – affecting nearly 33 million people and causing 345,000 deaths annually – yet, it is preventable with early detection and access to penicillin.
To help end the epidemic, Children’s National Health System has been awarded a $3.7 million grant from the American Heart Association (AHA) to launch a Rheumatic Heart Disease Center, with the goal of developing innovative strategies and economic incentives to improve the prevention and diagnosis of RHD in high-risk, financially disadvantaged countries and low-income communities across the United States.
Children’s National is one of four centers in the AHA’s Strategically Focused Children’s Research Network, which is dedicated to improving children’s heart health and reducing the global burden of cardiovascular disease and stroke. AHA selected Children’s for the grant based on its proven record of global collaboration to solve complex health issues and the potential impact of this research. The program will use Children’s robust telemedicine infrastructure to connect co-collaborators around the world, as well as train the next generation of globally minded cardiovascular researchers.
“While it’s often thought that we’ve already beaten rheumatic heart disease, data shows there’s nearly no decrease in mortality rates in low-income countries. The disease is endemic in Sub-Saharan Africa, and some poverty-stricken communities in the U.S. are hit nearly as hard,” said Craig Sable, M.D., associate division chief of cardiology. “We are thrilled to receive this funding from the AHA, which will help us close the research gap for this neglected disease and change the plight of millions of children around the world.”
Over the next four years, the Rheumatic Heart Disease Center, led by Children’s National Heart Institute experts Dr. Sable and Andrea Beaton, M.D., cardiologist, along with RHD leaders around the globe, will develop evidence-based strategies to strengthen the health system’s response to RHD through synergistic basic, clinical and population science research along the entire spectrum of the disease.

The Rheumatic Heart Disease Center, led by Children’s National Heart Institute experts Andrea Beaton, M.D., and Craig Sable, M.D., along with RHD leaders around the globe, will develop evidence-based strategies to strengthen the health system’s response to RHD.
The basic research project, led by James Dale, M.D., chief of the division of infectious disease at the University of Tennessee in Memphis, will work to better define the immune system response to Group A Streptococcal (GAS) infection, or strep throat, paving the way for vaccine development. In collaboration with a partner site in Cape Town, South Africa, experts will recruit 300 children ages 5-15 to participate for 24 months in a study capturing and classifying various strains of the GAS bacteria. Similar to the common flu, the strains of GAS bacteria vary from region to region and year to year. By identifying immune system targets, or how our bodies fight GAS, the research can inform the creation of effective and long-lasting vaccines.
Dr. Beaton will lead the clinical project that will work to improve understanding and detection of ARF, the precursor to RHD. According to Dr. Beaton, the current, outdated paradigm is that patients with RHD at one point experienced a full-blown episode of ARF – including fever, severe joint pains and rash. These symptoms should be unmistakable and prompt treatment, but in truth the disease remains vastly underdiagnosed in high-risk regions. Through an on-the-ground partnership with experts at Mulago National Referral Hospital in Uganda, the clinical project will work to enroll over 1,000 children ages 3-18 with more subtle symptoms, potentially suggestive of ARF, in order to paint a more accurate picture of the disease in Africa today.
“The gap between the low number of children diagnosed with ARF and the high number of young adults with advanced RHD remains one of the most challenging mysteries and barriers to improved RHD prevention,” said Dr. Beaton. “For the first time, we will systematically characterize the clinical, laboratory and echocardiographic features of ARF in low-resource settings, with the goal of developing a biological signature for ARF that can be translated into a diagnostic test and improve detection.”
Dr. Beaton expects that this research could benefit other related diseases too, such as kidney disease or serious skin infections.
The population research project, led by David Watkins, M.D., M.P.H., an expert in epidemiological and economic modeling at the University of Washington in Seattle, will work to build an economic case for prevention around the world, using the data from the basic and clinical work. The goal is to identify local gaps in delivery of health services for disease prevention and treatment and to measure the cost-effectiveness of RHD interventions, as well as the cost of inaction – especially as patients suffering from advanced RHD are often in the prime of their productive, adult lives. Researchers anticipate the findings will provide effective tools for addressing RHD in other endemic countries too.


For seven years, a Children’s National team has worked on new technologies to blunt the severity of rheumatic heart disease around the world, vastly improving patients’ chances of avoiding serious complications.
Rheumatic heart disease (RHD) is caused by repeated infections from the same bacteria that cause strep throat, which progressively lead to worsening inflammation of the heart’s valves with each successive infection. Over time, these valves thicken with scar tissue and prevent the heart from effectively pumping life-sustaining, oxygenated blood. The devastating condition, which was endemic in the United States before 1950, is now so rare that few outside the medical community have even heard of it. But in the developing world, explains Craig Sable, M.D., director of echocardiography and pediatric cardiology fellowship training and medical director of telemedicine at Children’s National Health System, RHD is nearly as common as HIV.
“RHD is the world’s forgotten disease,” Dr. Sable says. An estimated 32.9 million people worldwide have this condition, most of whom reside in low- to middle-income countries — places that often lack the resources to effectively diagnose and treat it.
Dr. Sable, Andrea Z. Beaton, M.D., and international colleagues plan to overturn this paradigm. For the last seven years, the team has worked on developing new technologies that could blunt the severity of RHD, vastly improving patients’ chances of avoiding its most serious complications.
At the heart of their approach is telemedicine — the use of telecommunications and information technology to provide clinical support for doctors and other care providers who often practice a substantial distance away. Telemedicine already has proven extremely useful within resource-rich countries, such as the United States, according to Dr. Sable. He and Children’s National colleagues have taken advantage of it for years to diagnose and treat pediatric disease from a distance, ranging from diabetes to asthma to autism. In the developing world, he says, it could be a game-changer, offering a chance to equalize healthcare between low- and high-resource settings.
In one ongoing project, a team led by Drs. Sable and Beaton is using telemedicine to screen children for RHD, a critical step to making sure that kids whose hearts already have been damaged receive the antibiotics and follow-up necessary to prevent further injury. After five years of working in Africa, the team recently expanded their project to Brazil, a country riddled with the poverty and overcrowding known to contribute to RHD.
Starting in 2014, the researchers began training four non-physicians, including medical technicians and nurses, to use handheld ultrasound machines to gather the precise series of heart images required for RHD diagnosis. They deployed these healthcare workers to schools in Minas Gerais, the second-most populous state in Brazil, to screen children between the ages of 7 and 18, the population most likely to be affected. With each worker scanning up to 30 children per day at 21 area schools, the researchers eventually amassed nearly 6,000 studies in 2014 and 2015.
Each night, the team on the ground transmitted their data to a cloud server, from which Children’s cardiologists, experts in RHD, and a regional hospital, Universidade Federal de Minas Gerais, accessed and interpreted the images.
“There was almost zero downtime,” Dr. Sable remembers. “The studies were transferred efficiently, they were read efficiently, and the cloud server allowed for easy sharing of information if there was concern about any questionable findings.”
In a study published online on November 4, 2016 in the Journal of Telemedicine and Telecare, Dr. Sable and colleagues reported the project’s success. Together, the team diagnosed latent heart disease in 251 children — about 4.2 percent of the subjects screened — allowing these patients to receive the regular antibiotics necessary to prevent further valve damage, and for those with hearts already badly injured to receive corrective surgery.
The researchers continued to collect data after the manuscript was submitted for publication. The team, which includes Drs. Bruno R. Nascimento, Adriana C. Diamantino, Antonio L.P. Ribeiro and Maria do Carmo P. Nunes, has screened a total of roughly 12,000 Brazilian schoolchildren to date.
Dr. Sable notes there is plenty of room for improvement in the model. For example, he says, the research team has not found a low-bandwidth solution to directly transmit the vast amount of data from each screening in real time, which has caused a slight slowdown of information to the hospital teams. The team eventually hopes to incorporate RHD screenings into annual health exams at local health clinics, sidestepping potential drawbacks of school day screenings.
Overall, being able to diagnose RHD using non-physicians and portable ultrasounds could eventually help Minas Gerais and additional low- to middle-income areas of the world where this disease remains endemic reach the same status as the United States and other resource-heavy countries.
“We’re putting ultrasound technology in the hands of people who otherwise wouldn’t have it,” says Dr. Sable, “and it could have a huge impact on their overall health.”
This work was supported by a grant from the Verizon Foundation and in-kind donations from General Electric and ViTelNet.
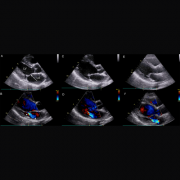
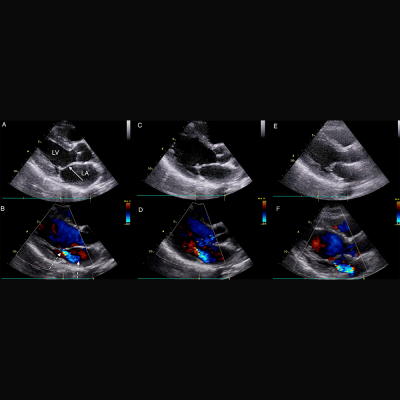
Parasternal long axis echocardiographic still frames in early systole in black and white and color Doppler of RHD-positive index case, sibling, and mother.
Siblings of children in Northern Uganda with latent rheumatic heart disease (RHD) are more likely to have the disease and would benefit from targeted echocardiographic screening to detect RHD before it causes permanent damage to their heart valves, according to an unprecedented family screening study.
RHD results from a cascade of health conditions that begin with untreated group A β-hemolytic streptococcal infection. In 3 percent to 6 percent of cases, repeat strep throat can lead to acute rheumatic fever. Almost half of children who experience acute rheumatic fever later develop chronic scarring of the heart valves, RHD. RHD affects around 33 million people and occurs most commonly in low-resource environments, thriving in conditions of poverty, poor sanitation, and limited primary healthcare. Treating streptococcal infections can prevent a large percentage of children from developing RHD, but these infections are difficult to diagnose in low-resource settings.
Right now, kids with RHD often are not identified until they reach adolescence, when the damage to their heart valves is advanced and severe cardiac symptoms or complications develop. In such countries, cardiac specialists are rare, and intervention at an advanced stage is typically too expensive or unavailable. Echocardiographic screening can “see” RHD before symptoms develop and allow for earlier, more affordable, and more practical intervention. A team led by Children’s National Health System clinicians and researchers conducted the first-ever family echocardiographic screening study over three months to help identify optimal strategies to pinpoint the families in Northern Uganda at highest RHD risk.
“Echocardiographic screening has the potential to be a powerful public health strategy to lower the burden of RHD around the world,” says Andrea Beaton, M.D., a cardiologist at Children’s National and the study’s senior author. “Finding the 1 percent of vulnerable children who live in regions where RHD is endemic is a challenge. But detecting these silent illnesses would open the possibility of providing these children monthly penicillin shots – which cost pennies and prevent recurrent streptococcal infections, rheumatic fever, and further valve damage.”
The research team leveraged existing school-based screening data in Northern Uganda’s Gulu District and recruited 60 RHD-positive children and matched them with 67 kids attending the same schools who were similar in age and gender but did not have RHD. After screening more than 1,000 parents, guardians, and first-degree family members, they found that children with RHD were 4.5 times as likely to have a sibling who definitely had RHD.
“Definite RHD was more likely to be found in mothers, with 9.3 percent (10/107 screened) having echocardiographic evidence of definite RHD, compared to fathers 0 percent (0/48 screened, p = 0.03), and siblings 3.3 percent (10/300 screened, p = 0.02),” writes lead author Twalib Aliku, School of Medicine, Gulu University, and colleagues. “There was no increased familial, or sibling risk of RHD in the first-degree relatives of RHD-positive cases (borderline & definite RHD) versus RHD-negative cases. However, RHD-positive cases had a 4.5 times greater chance of having a sibling with definite RHD (p = 0.05) and this risk increased to 5.6 times greater chance if you limited the comparison to RHD-positive cases with definite RHD (n = 30, p = 0.03.”
The paper, “Targeted Echocardiographic Screening for Latent Rheumatic Heart Disease in Northern Uganda,” was published recently by PLoS and is among a dozen papers published this year about the group’s work in Africa, done under the aegis of the Children’s Research Institute global health initiative.
The World Health Organization previously has prioritized screening household contacts when an index case of tuberculosis (TB) is identified, the authors note. Like TB, RHD has a strong environmental component in that family members are exposed to the same poverty, overcrowding, and circulating streptococcal strains. In a country where the median age is 15.5, it is not practical to screen youths without a detailed plan, Dr. Beaton says. Additional work would need to be done to determine which tasks to shift to nurses, who are more plentiful, and how to best leverage portable, hand-held screening machines.
“Optimal implementation strategies, the who, when, in what setting, and how often to screen, have received little study to date, yet these details are critical to developing cost-effective and sustainable screening programs,” Aliku and co-authors write. “Our study suggests that siblings of children identified with latent RHD are a high-risk group, and should be prioritized for screening.”
Related resources: Research at a Glance

|
What’s Known What’s New Questions for Future Research Source: “Targeted Echocardiographic Screening for Latent Rheumatic Heart Disease in Northern Uganda: Evaluating Familial Risk Following Identification of an Index Case.” T. Aliku, C. Sable, A. Scheel, A. Tompsett, P. Lwabi, E. Okello, R. McCarter, M. Summar, and A. Beaton. Published online by PLoS June 13, 2016. |

July 20, 2016 – Utility of fetal magnetic resonance imaging in assessing the fetus with cardiac malposition
Abnormal cardiac axis and/or malposition can trigger an evaluation of fetuses for congenital heart disease. A research team led by Mary T. Donofrio, MD, director of the Fetal Heart Program at Children’s National Health System, sought to examine how fetal magnetic resonance imaging (fMRI) – might complement obstetrical ultrasound or fetal echocardiography (echo) – in defining etiology. The team reviewed 42 fetuses identified as having abnormal cardiac axis and/or malposition by fetal ultrasound and echo. While 55 percent of cases (23) had extracardiac anomalies, 29 percent (12) were reassigned by fMRI. fMRI findings were confirmed in 8 of these 12 cases postnatally.
June 13, 2016 – Targeted echocardiographic screening for latent rheumatic heart disease in Northern Uganda
Echocardiographic screening to detect latent rheumatic heart disease (RHD) has the potential to reduce the burden of disease, however additional research is needed to develop sustainable public health strategies. Some 33 million people, many living in low-resource environments, have RHD. What’s more, relatives of children with latent RHD may be at risk for developing the chronic heart condition. The research team found that siblings of children who were RHD-positive were more likely to have RHD, underscoring the importance of screening brothers and sisters of a child with confirmed RHD.
April 3, 2016 – Chest pain in children – the charge implications of unnecessary referral
While pediatricians are responsible for triaging chest pain complaints, questions linger about the best approach to reassure patients whose conditions are benign as well as how to best identify patients whose chest pain warrants further evaluation and testing. The study sought to assess how many patients with chest pain were inappropriately referred and found that chest pain due to cardiac disease is very rare in children. Thus, children whose chest pain is not accompanied by cardiac red flags can be managed safely by their pediatrician.
April 2, 2016 – Hemodynamic consequences of a restrictive ductus arteriosus and foramen ovale in fetal transposition of TGA
Dextro-transposition of the great arteries (d-TGA) occurs when the position of the main pulmonary artery and the aorta – the two main arteries that carry blood out of the heart – are switched. Newborns with d-TGA are at risk for compromise due to foramen ovale (FO) closure and pulmonary vascular abnormalities. One such fetus seen at 22 weeks of gestational age had a hypermobile, unrestrictive FO and small ductus arteriosus (DA) with bidirectional flow. By the 32 week, however, the DA was small with restrictive bidirectional flow. Doppler imaging showed reversed flow in the left pulmonary artery. By the 38th gestational week, the FO was closed, the left atrium/ventricle were dilated, and the DA was tiny. Within 30 minutes after birth, a balloon atrial septostomy was performed, and the infant later underwent surgical repair.

