In a first-of-its-kind clinical trial, researchers found that intravenous therapies made from virus-specific T-cells (VST) can effectively treat immunocompromised pediatric patients, far surpassing the current standard of care, according to new research published in Nature Communications.
More than 60% of patients in the phase 2 clinical trial led by investigators from Children’s National Hospital and Huntsman Cancer Institute responded to the innovative VST therapy. This new treatment uses blood from healthy donors to manufacture a highly specialized immune therapy that, when given to immune-compromised patients, prompts their immune system to fight off potentially life-threatening viruses, including cytomegalovirus, Epstein-Barr and adenovirus. Without this therapy, estimates suggest that less than 30% of patients would recover, using standard protocols.
“A vast majority of our patients not only responded to the therapy, but they were able to come off their antivirals, which come with extensive side effects,” said Michael Keller, M.D., the paper’s first author and the Translational Research Laboratory director at the Children’s National Cell Enhancement and Technologies for Immunotherapy (CETI) program. “This promising data suggests hope for patients with rare immune-compromising diseases that leave them vulnerable to so much in the world.”
The study brings together experts from the Pediatric Transplantation and Cell Therapy Consortium (PTCTC) and the Primary Immune Deficiency Treatment Consortium (PIDTC) to create the first multi-center, pediatric-consortium trial of adoptive T-cell therapies for viruses. It also represents one of the first to include critically ill patients, who are often excluded from research.
Children’s National leads the way
Working alongside Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research (CCIR), Dr. Keller and the CCIR team helped build an internationally recognized program, pioneering therapies to prevent complications from viral infections in immunocompromised patients. This includes patients with congenital immune deficiency and others who have undergone bone marrow transplantation for malignancies or non-malignant conditions, such as sickle cell disease.
While doctors can treat some immune-compromised patients for infections with standard antivirals, a small fraction don’t respond. Children’s National is one of a handful of hospitals in the country that has options. Over the last several decades, researchers have found ways to develop VST therapies made from banked T-cells, a more advanced application of how donated red blood cells are used to treat anemia.
In 2017, Drs. Keller and Bollard started collaborating with Michael Pulsipher, M.D.—now with Intermountain Primary Children’s Hospital and the Huntsman Cancer Institute at the University of Utah—to create a multi-institute clinical study. They combined the expertise at Children’s National in producing and banking cell therapy products with the community built around the PTCTC. Ultimately, they launched a clinical trial that was open to 35 centers in the U.S., enrolling 51 patients at 22 hospitals from 2018-2022.
“We wanted to prove that this potentially life-saving therapy could be given safely at regional pediatric centers that had never been able to use this approach before,” said Dr. Pulsipher, who served as the study’s co-principal investigator with Dr. Keller. “We united top experts in this area from the PTCTC and PIDTC and successfully treated some of the most challenging patients ever treated with this approach. Our findings helped define who can benefit the most from this therapy, paving the way for commercial development.”
The Good Manufacturing Practices (GMP) laboratory at Children’s National, led by Patrick Hanley, Ph.D., provided suitable VST therapies for 75 of 77 patients who requested to join the study. Clinical responses were achieved in 62% of patients who underwent stem cell transplants and in 73% of patients who were treated with VST and evaluated one month after their infusion. The paper laid out risks and clinical factors impacting outcomes when third-party donors are used to manufacture the VST therapies.
What’s ahead
Given that researchers are only beginning to develop cell therapies, work remains to understand the many ways they interact with the immune system. In a separate paper also recently published in Nature Communications, members of the multi-institute team documented a case of an infant with severe combined immune deficiency, who faced extremely rare side effects when the VST treatment interfered with her donor bone marrow graft. The case led the team to work with the Food and Drug Administration to identify criteria for VST donors enrolled in this study to mitigate complications.
In the decade ahead, Dr. Bollard sees promise in cell therapies for patients with cancer, immune deficiencies after transplant and dozens of other disorders, including genetic and autoimmune diseases. “Future studies will continue to look at ways to optimize the manufacturing, the administration and the long-term outcomes for these therapies—and to enhance the lifelong impact on our patients,” she said. “When we pair human ingenuity with the power of technology, I see tremendous potential.”
Acknowledgments: This study was funded with a nearly $5 million grant from the California Institute of Regenerative Medicine and was run through the operations center at the Children’s Hospital of Los Angeles, where Dr. Pulsipher was formerly on faculty.
Trial participant Mia Maric is measured by Dr. Andrew Dauber.
Researchers from Children’s National Hospital presented findings from the first clinical trial of the medication vosoritide for children with hypochondroplasia – a rare genetic growth disorder. The results were presented at the 2024 American College of Medical Genetics and Genomics (ACMG) Annual Clinical Genetics Meeting.
Recently approved to increase linear growth and open growth plates in children with achondroplasia, vosoritide is a C-type natriuretic peptide analog that binds its receptor on chondrocytes, leading to increased chondrocyte proliferation and differentiation by inhibiting the ERK1/2-MAPK pathway.
“Vosoritide directly targets the pathway in the growth plate that is affected by the genetic mutation causing hypochondroplasia,” said Andrew Dauber M.D., M.M.Sc., chief of Endocrinology at Children’s National and lead author of the study.
During the phase 2 trial, researchers found vosoritide increased the growth rate in children with hypochondroplasia, allowing them to grow on average an extra 1.8 cm per year.
Ivan Maric’s 11-year-old daughter, Mia, has been participating in the trial for the last 18 months. In 2022, they moved from Croatia to be part of the study.
“This has been life-changing for Mia,” Maric said. “Soon after receiving the initial doses, we immediately noticed growth. Now, she can independently manage everyday tasks such as washing her hair and reaching the sink to wash her hands.”
Vosoritide treatment may work as a precision therapy to improve growth in multiple genetic conditions that interact with the ERK1/2-MAPK pathway.
“This study provides a proof of principle that this medicine will work for these children and supports further research in this area,” said Dr. Dauber. “I was excited to see how well tolerated the medication was and how some patients had excellent responses.”
This clinical trial funded by BioMarin is the first-of-its-kind to treat children with genetic short stature who do not have achondroplasia. Other growth-related conditions included in this phase 2 trial were Noonan syndrome, NPR2 mutations and Aggrecan mutations.
Additional authors from Children’s National: Anqing Zhang, Ph.D., Roopa Kanakatti Shankar, M.D., Kimberly Boucher, R.N., Tara McCarthy, B.A., Niusha Shafaei, B.A., Raheem Seaforth, B.A., Meryll Grace Castro, M.S., and Niti Dham, M.D.


FACE-TC effectively increases communication between adolescents with cancer and their families about the patients’ preferences.
Talking about death and dying is taboo. Some families believe it is their role alone to make end-of-life healthcare decisions or they may believe pediatric advance care planning is against their religion.
In a recent trial, Maureen Lyon, Ph.D., a clinical health psychologist at Children’s National Hospital and lead author of the study, analyzed the value of high-quality pediatric advance care planning and how this enabled families to know their adolescents’ end-of-life treatment preferences.
This is the first fully powered randomized controlled trial to focus on adolescents with cancer and their engagement with their families in pediatric advance care planning conversations.
Some physicians believe it is not their role to discuss the “what ifs.” Others report that they do not have the training or time to do so. As a result, in clinical practice, adolescents living with a serious illness rarely have documented advance care plans. The default is to provide intensive treatments that potentially increase suffering.
“Despite cancer being the leading cause of disease-related death in adolescents, conversations about goals of care and documentation of end-of-life care and treatment preferences for adolescents with cancer are not a routine and standard part of care,” Dr. Lyon said.
Family-centered advance care planning for teens with cancer (FACE-TC) effectively increases communication between adolescents with cancer and their families about the patients’ end-of-life preferences. This meets the first challenge of pediatric advance care planning – knowledge of patient’s preferences.
This low-tech intervention commits to more deeply respecting adolescents with cancer, integrating them into health care decision-making and giving them some control in a low control situation.
“FACE-TC strengthens communication between adolescents with cancer and their families about adolescents’ understanding of their illness, their hopes and fears, their goals of care and their end-of-life treatment preferences,” Dr. Lyon added. “With increased access to palliative care services and pediatric advance care planning, families may better understand that stopping intensive medical interventions when their child is dying is not giving up, but rather choosing how best to spend the final days of one’s life.”
Dr. Lyon and the team at Children’s National have pioneered this effort to give seriously ill adolescents a voice and help families break the ice so they know what their child would want if the worst were to happen. The team also aims to provide an extra level of support for busy clinicians so the first conversation about goals of end-of-life care does not happen in the intensive care unit.
You can read the full trial, An Intervention in Congruence for End-of-Life Treatment Preference: A Randomized Trial, in Pediatrics.
You can also read the last manuscript from this clinical trial, Effect of the Family-Centered Advance Care Planning for Teens with Cancer Intervention on Sustainability of Congruence About End-of-Life Treatment Preferences, in JAMA Network.
The American Society of Hematology Research Collaborative (ASH RC) has announced the first 10 clinical research consortia to join the ASH RC Sickle Cell Disease Clinical Trials Network. Children’s National Hospital will be one of the clinical trials units to serve in the DMV Sickle Cell Disease Consortium (DMVSCDC).
The sites will be able to enroll children and adults living with sickle cell disease (SCD) within their patient populations in clinical trials as part of an unprecedented national effort to streamline operations and facilitate data sharing to expedite the development of new treatments for this disease.
“As part of the ASH RC SCD clinical trials network, we will learn regionally and nationally how sickle cell patients respond differently to therapies, hopefully giving us clues to provide more successful targeted and individualized treatments that will improve the morbidity and mortality in sickle cell disease patients,” said Andrew Campbell, M.D., director of Comprehensive Sickle Cell Disease Program at Children’s National.
SCD is a chronic, progressive, life-threatening, inherited blood disorder that affects more than 100,000 Americans and an estimated 100 million persons worldwide. Clinical trials hold incredible promise for the development of much-needed new treatments, and possibly even a cure. While there are currently only four U.S. Food and Drug Administration (FDA)-approved drugs to treat the disease, there is a robust SCD drug development pipeline that will drive demand for clinical trials to a new level, providing a prime opportunity to advance treatment and care of those affected by SCD.
“We are proud that the DMV Sickle Cell Disease Consortium will contribute regionally, allowing our patients and families to benefit from new clinical trials investigating new therapies that may improve the clinical course and quality of life of patients living with sickle cell disease in the DMV region,” Dr. Campbell added. “We will also have an integrated Community Advisory Board who will continue to provide guidance and expertise for our consortium including patients, families and caregivers.”
Read the full list of other hospitals joining the network.


Roger Packer, M.D., senior vice president of the Center for Neurosciences and Behavioral Medicine at Children’s National Hospital, will speak at a series of symposiums in the next couple of months.
Most recently, he presented on pediatric brain tumor trials at a webinar hosted by the American Brain Tumor Association titled “Clinical Trials – Paving the Way Forward.” In case you missed it, you can watch it here.
For details on more upcoming presentations, see below:
On Friday, May 14, Dr. Packer will speak at the Cure Search for Children’s Cancer’s ‘Blurred Lines: Therapeutic vs. Research-only Biopsies,’ a session highlighting technologies, including liquid biopsies and single-cell sequencing, that have the potential to allow researchers to collect more data while decreasing the amount of tissue needed from solid tumor biopsies.
On Friday, May 28, he will give a virtual keynote address at the Dmitry Rogachev National Medical Research Center of Pediatric Hematology, Oncology and Immunology during their “Pediatric oncology, hematology and immunology in 21st century: From research to clinical practice” online presentation. Dr. Packer will co-chair the session on central nervous system tumors and present on “CNS tumors: Major advances in neuro-oncology in last 10 years.”
And at the 50th Golden Anniversary Meeting of the Child Neurology Society, taking place September 29 to October 2, Dr. Packer will lead a symposium on new therapies for childhood medulloblastoma — the most common malignant brain tumor in children. Here, he will receive a recognition during the society’s annual gala honoring the “Founders of Child Neurology,” for his contribution in a new book in which Dr. Packer has a chapter outlining the history of child neurologists in the field of pediatric neuro-oncology.
Marrow replaced with acute lymphoblastic leukemia.
According to a study that accrued over 9,000 patients, a new approach to maintenance therapy lessens the burden of treatment and potential toxicity in children experiencing the most common cancer — B-acute lymphoblastic leukemia (B-ALL). The average-risk (AR) B-ALL subset of patients demonstrated an overall five-year survival rate of 98% despite less frequent chemotherapy pulses. Researchers from Children’s National Hospital led the 10-year study published on Jan. 7, 2021, in the Journal of Clinical Oncology.
This phase III clinical trial, which opened at over 200 centers, helped inform an alternative maintenance therapy with less frequent administration of vincristine and dexamethasone. These standard drugs are part of a multiagent treatment approach used to treat acute lymphoblastic leukemia (ALL).
“For decades, the common maintenance therapy approach [within the Children’s Oncology Group] was administering vincristine or steroid pulses every four weeks. The steroids can trigger disruptive behaviors like moodiness, sleep disturbance, food cravings, poor school attendance or physical aggression and vincristine can cause declines in fine motor and sensory-perceptual performance,” said Anne Angiolillo, M.D., lead author of the study and director of the Leukemia and Lymphoma Program at Children’s National. “We can now lessen the burden of this therapy while still maintaining excellent outcomes, which is a huge benefit to our patients and their families.”
The findings suggest that the decreased frequency of both vincristine and dexamethasone pulses every four weeks to every 12 weeks alleviates the therapy burden and reduces toxicity, potentially improving children’s quality of life.
Simultaneously, the researchers tried increasing the starting dose of oral methotrexate, a standard chemotherapy drug, given once weekly in the maintenance phase to see if it would improve the five-year disease-free survival rate, but, according to the data, it did not improve outcomes.
The world’s largest organization devoted exclusively to pediatric cancer research, the Children’s Oncology Group (COG), adopted the approach of less frequent pulses into the frontlines of their new B-ALL trials, given the study’s findings, to help decrease the therapy burden for patients and their families.
“I am very excited that the results of AALL0932 [the clinical trial] will have a major effect on the schedule of maintenance therapy for children with standard and high-risk B acute lymphoblastic leukemia in all future COG therapeutic trials,” said Dr. Angiolillo.
Dr. Angiolillo, and co-author Reuven Schore, M.D., pediatric oncologist at Children’s National were the chair and vice-chair of the clinical trial, respectively. Dr. Schore is also a member of the Leukemia and Lymphoma Program at Children’s National.
ALL can progress quickly, affect the bone marrow and the blood, including B cells and T cells. Among the children with ALL, approximately 55% comprise of the newly diagnosed National Cancer Institute (NCI) standard-risk (SR) B-ALL.
The study enrolled 9,229 patients with B-ALL between August 2010 and March 2018. Only 2,364 patients classified as average-risk received a random assignment to one of the four maintenance arms at the start of maintenance therapy. The researchers administered either vincristine/dexamethasone pulses every 12 weeks or every four weeks and a starting dose of once-weekly oral methotrexate of 20 mg/m2 or 40 mg/m2 during the maintenance phase.
“This trial establishes that with improved risk stratification utilizing blast cytogenetics and rate of response, a relatively low-intensity premaintenance backbone with a three-drug induction, and lower exposure to chemotherapy in maintenance, results in outstanding outcomes,” said Angiolillo et al.


A new grant will help to finalize development of the Pediatric PUMA-G System, the world’s first and only ultrasound-based procedure for placing feeding tubes into the stomach.
Researchers at Children’s National Hospital have received grant funding from the National Institute of Diabetes and Digestive and Kidney Diseases, within the National Institutes of Health (NIH), to finalize development of the Pediatric PUMA-G System, the world’s first and only ultrasound-based procedure for placing feeding tubes into the stomach. The funding will also support the first clinical trial of this technology in pediatric patients.
“Children’s National was chosen because we have a strong record of innovating pediatric devices and surgical procedures through the Sheikh Zayed Institute and we have a busy clinical interventional radiology service,” says Karun Sharma, M.D., Ph.D., director of Interventional Radiology and associate director of clinical translation at the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI) at Children’s National. “We are proud to be a part of this collaboration that will potentially help improve care of pediatric patients who cannot tolerate feeding by mouth.”
The feeding tubes are vital for children who cannot eat or swallow and require liquid nutrition (known as enteral feeding). Common feeding tube placement procedures for children may expose them to risks from invasive surgical tools or from ionizing radiation, which may lead to cancer in young patients at elevated rates. The PUMA-G System is less invasive and uses ultrasound to help physicians image the body during the procedure.
The grant, totaling $1.6M, will clinically evaluate the Pediatric PUMA-G System in collaboration with CoapTech, a biotechnology medical device company and two other premier pediatric medical centers — New York-Presbyterian Morgan Stanley Children’s Hospital and Children’s Hospital of Philadelphia.
Researchers found that patients with localized pediatric renal cell carcinoma have excellent short-term outcomes without adjuvant therapy.
Although renal cell carcinoma (RCC) is the second most common kidney cancer diagnosed in children and adolescents, guidance regarding its clinical management has been confined to retrospective case series, which were limited by reporting bias, varied treatment approaches and a lack of central pathology review to confirm the diagnosis.
Research conducted by the Children’s Oncology Group (COG) and led by Jeffrey Dome, M.D., Ph.D., vice president of the Center for Cancer and Blood Disorders at Children’s National Hospital, found that patients with localized pediatric RCC have excellent short-term outcomes without adjuvant therapy with 4-year overall survival estimates of 96% for patients with stage I disease, 100% for patients with stage II disease and 88% for patients with stage III disease.
“The results of this study provide important practical insights into the management of pediatric RCC,” said Dr. Dome. “Oncologists now have validation that a surgery-only approach is appropriate management for the majority of children and adolescents with RCC.”
“The results of this study provide important practical insights into the management of pediatric RCC,” said Jeffrey Dome, M.D., Ph.D.
The excellent survival in patients with stage III disease held up even in those with tumor involvement of regional lymph nodes, a finding that differs from adult RCC. However, patients with metastatic disease (stage IV), had a 4-year overall survival estimate of only 29%, demonstrating the need to find active treatments for this group. Outcomes varied according to tumor histological subtype. Nearly all recurrences occurred in patients with the translocation histology and renal medullary carcinoma; recurrences were rare in other subtypes.
A follow-up study called AREN1721 is now open in the Children’s Oncology Group and adult cancer cooperative groups that participate in the National Clinical Trials Network. This study involves a comparison of two treatment regimens for metastatic or unresectable “translocation” renal cell carcinoma, the most common subtype of renal cell carcinoma in children, adolescents and young adults. The treatment regimens will include nivolumab, a PD1 immune checkpoint inhibitor, with or without axitinib, a tyrosine kinase inhibitor that targets vascular endothelial growth factor receptor (VEGFR).

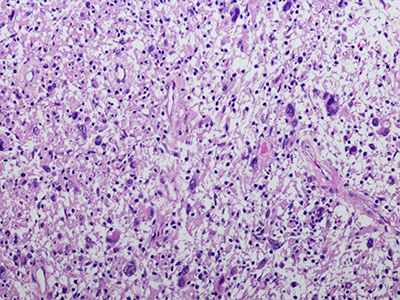
Intermediate magnification micrograph of Ewing sarcoma in lung.
Despite advances in chemotherapy, the outcome for metastatic or relapsed Ewing sarcoma (ES) is dismal. ES harbors a pathognomonic translocation EWS-FLI1, leading to an oncogenic fusion protein that drives its development and for years has been considered an undruggable target. TK216 is a unique, investigational agent that targets EWS-FLI1 by disrupting its binding to RHA, a protein partner needed for the activity of EWS-FLI1, and one of the first in class to do so. In pre-clinical models of ES, there was cell death and inhibition of tumor growth which was potentiated with vincristine.
Study TK216-01 is a Phase 1 study of TK216 in patients with relapsed or refractory Ewing sarcoma currently open at a limited number of sites. The initial Phase 1 data demonstrates this drug has been generally well tolerated with encouraging preliminary data in patients. The study is currently in the expansion cohort using the recommended phase 2 dose of TK216 in combination with vincristine and is open to enrollment at Children’s National.
“There was interesting preliminary data presented at the CTOS meeting last November,” says AeRang Kim, M.D., Ph.D., a pediatric oncologist at Children’s National and the study’s principal investigator. “This really is a first-in-class that targets this specific translocation which makes it an exciting option for this patient group.”
Children’s National Hospital is the only pediatric center in the Washington, D.C., region to offer this trial.
TK216 in Patients with Relapsed or Refractory Ewing Sarcoma
For more information about this trial, contact:
Ann Liew, M.S., CCRP
202-476-6755
aliew@childrensnational.org
Click here to view Open Phase 1 and 2 Cancer Clinical Trials at Children’s National.
The Children’s National Center for Cancer and Blood Disorders is committed to providing the best care for pediatric patients. Our experts play an active role in innovative clinical trials to advance pediatric cancer care. We offer access to novel trials and therapies, some of which are only available here at Children’s National. With research interests covering nearly every aspect of pediatric cancer care, our work is making great advancements in childhood cancer.
Each year, about 9,000 new patients are diagnosed with Hodgkin lymphoma, 10-15% of them children.
Each year, about 9,000 new patients are diagnosed with Hodgkin lymphoma, 10-15% of them children. Despite a relatively high cure rate for children with Hodgkin lymphoma, there are many debilitating long-term side effects of the treatments currently used. Additionally, 15-20% of children have a relapse and only half of them experience a long-term cure. Diffuse large B cell Lymphomas are another type of aggressive lymphoma that are difficult to cure, especially when they do not respond to upfront chemotherapy (refractory). Patients who experience relapse have to undergo more intensive chemotherapy followed by autologous stem cell transplantation and yet often times their lymphoma comes back.
Physicians at Children’s National Hospital, in partnership with the Huntsman Cancer Institute at the University of Utah School of Medicine, are enrolling patients in a clinical trial to test the safety of administering PD-1 inhibitor Nivolumab given prior to and following the infusions of the patients’ own TAA-T cells which have been trained to target tumor cells in the laboratory. Nivolumab is currently approved by the FDA for relapsed Hodgkin lymphoma. Nivolumab acts by unleashing the brakes put on by the lymphoma cells, and by doing so, Nivolumab allows the immune system to overcome the tumor’s escape mechanism.
“We believe that if our T cells are deemed safe when given in combination with already approved drugs, we may be able to impact multiple lives and reduce long-term toxicities from conventional chemotherapies,” said Hema Dave, M.D., an oncologist at Children’s National. “We’re hopeful that combination immunotherapies will produce more durable responses than when immunotherapies are given alone as a single agent and, additionally, that they will reduce the use of cytotoxic chemotherapy.”
The investigators will collect blood from the patients to isolate peripheral blood mononuclear cells. They will then make special cells called dendritic cells to stimulate the T cells. Then they will add special mixtures of tumor proteins WT1, PRAME and Survivin and provide a cytokine milieu favorable to T cell expansion/activation, inducing selective expansion of T cells targeted to kill tumor cells. This process trains the T cells to recognize the tumor proteins and become specialized TAA-T cells. The cells will be grown and frozen until ready for use. While the T cells are growing, the patients will be given Nivolumab.
“We’re really trying to test if priming the patients with Nivolumab will make their T cells more effective when they get infused,” says Dr. Dave. “The Nivolumab will help prepare the immune system. Then, when we infuse the T cells, our hope is that the environment is primed for the T cells to expand, grow and work to attack the cancer. If we can prime the immune system and make it more conducive for the T cells, then maybe they will have a better chance to get to the lymphoma cells and thus have a more sustained response.”
Patients will then receive two infusions of the TAA-T cells and be monitored for side effects. The anticipated enrollment is 18 patients over the next 2-3 years. If there is a positive response in patients enrolled in this safety trial, it could expand to test for efficacy of the novel combination immunotherapy.
For more information about this trial, contact:
Hema Dave, M.D.
202-476-6397
hkdave@childrensnational.org
Fahmida Hoq, MBBS, MS
202-476-3634
fhoq@childrensnational.org
Click here to view Open Phase 1 and 2 Cancer Clinical Trials at Children’s National.
The Children’s National Center for Cancer and Blood Disorders is committed to providing the best care for pediatric patients. Our experts play an active role in innovative clinical trials to advance pediatric cancer care. We offer access to novel trials and therapies, some of which are only available here at Children’s National. With research interests covering nearly every aspect of pediatric cancer care, our work is making great advancements in childhood cancer.
Children’s National Hospital collects patients’ blood, extracts T-cells and replicates them in the presence of specific proteins found on cancer cells which, in essence, teaches the T-cells to target specific tumor markers. Training the T-cells, growing them to sufficient quantities and ensuring they are safe for administration takes weeks. But when patients return to the outpatient clinic, their T-cell infusion lasts just a few minutes.
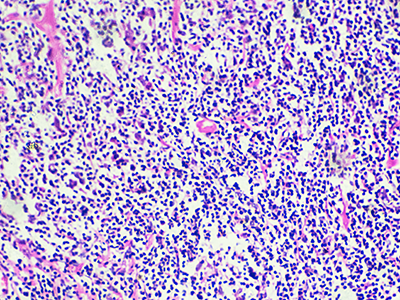
For the third consecutive year, Children’s National was selected to compete in STAT Madness, an annual bracket-style competition that chooses the year’s most impactful biomedical innovation by popular vote. Children’s entry, “Immunotherapy of relapsed and refractory solid tumors with ex vivo expanded multi-tumor associated antigen specific cytotoxic T lymphocytes,” uses the body’s own immune system to attack and eliminate cancer cells in pediatric and adult patients with solid tumor malignancies.
In 2018, Children’s first-ever STAT Madness entry advanced through five brackets in the national competition and, in the championship round, finished second. That innovation, which enables more timely diagnoses of rare diseases and common genetic disorders, helping to improve kids’ health outcomes around the world, also was among four “Editor’s Pick” finalists, entries that spanned a diverse range of scientific disciplines.
An estimated 11,000 new cases of pediatric cancer were diagnosed in children 14 and younger in the U.S. in 2019. And, when it comes to disease, cancer remains the leading cause of death among children, according to the National Institutes of Health. An enterprising research team led by Children’s National faculty leveraged T-cells – essential players in the body’s immune system – to treat pediatric and adult patients with relapsed or refractory solid tumors who had exhausted all other therapeutic options.
“We’re using the patient’s own immune system to fight their cancer, rather than more traditional chemotherapy drugs,” says Catherine M. Bollard, M.D., director of the Center for Cancer & Immunology Research at Children’s National and co-senior author of the study. “It’s more targeted and less toxic to the patient. These T-cells home in on any cancer cells that might be in the body, allowing healthy cells to continue to grow,” Dr. Bollard adds.
That means patients treated in the Phase I, first-in-human trial didn’t lose their hair and weren’t hospitalized for the treatment. After a quick clinical visit for their treatment, they returned to normal activities, like school, with good energy levels.
“With our specially trained T-cell therapy, many patients who previously had rapidly progressing disease experienced prolonged disease stabilization,” says Holly J. Meany, M.D., a Children’s National oncologist and the study’s co-senior author. “Patients treated at the highest dose level showed the best clinical outcomes, with a six-month, progression-free survival of 73% after tumor-associated antigen cytotoxic T-cell (TAA-T) infusion, compared with 38% with their immediate prior therapy.”
The multi-institutional team published their findings from the study online July 29, 2019, in the Journal of Clinical Oncology.
“Our research team and our parents are delighted that some patients treated in our study continue to do well following T-cell therapy without additional treatment. In some cases, two years after treatment, patients do not appear to have active disease and are maintaining an excellent quality of life,” says Amy B. Hont, M.D., the study’s lead author. “One of these was a patient whose parents were told his only other option was palliative care. Our innovation gives these families new hope,” Dr. Hont adds.
The 2020 STAT Madness #Core64 bracket opened March 2, and the champion will be announced April 6.
In addition to Drs. Hont, Meany and Bollard, Children’s National co-authors include C. Russell Cruz, M.D., Ph.D., Robert Ulrey, MS, Barbara O’Brien, BS, Maja Stanojevic, M.D., Anushree Datar, MS, Shuroug Albihani, MS, Devin Saunders, BA, Ryo Hanajiri, M.D., Ph.D., Karuna Panchapakesan, MS, Payal Banerjee, MS, Maria Fernanda Fortiz, BS, Fahmida Hoq, MBBS, MS, Haili Lang, M.D., Yunfei Wang, DrPH, Patrick J. Hanley, Ph.D., and Jeffrey S. Dome, M.D., Ph.D.; and Sam Darko, MS, National Institute of Allergy and Infectious Diseases.
Financial support for the research described in this post was provided by the Children’s National Hospital Heroes Gala, Alex’s Army Foundation, the Children’s National Board of Visitors and Hyundai Hope on Wheels Young Investigator Grant to Support Pediatric Cancer Research, the Children’s National Research Institute Bioinformatics Unit, the Clinical and Translational Science Institute and the National Institutes of Health under award No. UL1-TR001876.
Malignant peripheral nerve sheath tumors (MPNST) are aggressive soft tissue sarcomas and the most common malignancy associated with neurofibromatosis type 1 (NF1).
Malignant peripheral nerve sheath tumors (MPNST) are aggressive soft tissue sarcomas and the most common malignancy associated with neurofibromatosis type 1 (NF1). Half of all MPNST are seen in NF1 patients, and MPNST is a leading cause of mortality in young patients with NF1. Researchers led by AeRang Kim, M.D., Ph.D., a pediatric oncologist at Children’s National Hospital, are now searching for a medical treatment for this rare disease that currently has dismal survival rates.
“Through consortia efforts, we’ve been able to open and accrue in single histology trials of really rare diseases such as MPNST for which there are no known curative therapies other than surgery, and surgery is very difficult or not feasible in many patients,” says Dr. Kim, the principal investigator for the SARC031 trial sponsored by the Sarcoma Alliance for Research through Collaboration. “In this trial in particular, our hope is to find a new therapy that will benefit patients with MPNST for which we have no known effective medical therapies.”
Using a combination of drugs that target specific pathways involved in MPNST growth, Dr. Kim and colleagues at four other institutions offering the SARC031 trial will monitor patients to see if the drugs shrink, slow down or stop the growth of MPNSTs. Based on preclinical data demonstrating substantial MPNST shrinkage in mice treated with a combination of MEK and mTOR inhibitors, SARC031 is a trial of the MEK inhibitor selumetinib in combination with the mTOR inhibitor sirolimus for patients with unresectable or metastatic MPNST. The primary objective is to determine the clinical benefit of the combination.
SARC031: A Phase 2 Trial of the MEK Inhibitor Selumetinib (AZD6244 Hydrogen Sulfate) in Combination with the mTOR Inhibitor Sirolimus for Patients with Unresectable or Metastatic Malignant Peripheral Nerve Sheath Tumors
For more information about this trial, contact:
AeRang Kim, M.D., Ph.D.
202-476-2800
AeKim@childrensnational.org
Click here to view Open Phase 1 and 2 Cancer Clinical Trials at Children’s National.
The Children’s National Center for Cancer and Blood Disorders is committed to providing the best care for pediatric patients. Our experts play an active role in innovative clinical trials to advance pediatric cancer care. We offer access to novel trials and therapies, some of which are only available here at Children’s National. With research interests covering nearly aspect of pediatric cancer care, our work is making great advancements in childhood cancer.



“The T cell immunotherapy regimen resulted in prolonged disease stabilization in patients who previously experienced rapid tumor progression,” says Holly Meany, M.D. “The therapy could prove to be an important component of immunotherapy for patients with solid tumor malignancies.”
In a study published in the Journal of Clinical Oncology, researchers from Children’s National Health System uncovered tumor-associated antigen cytotoxic T cells (TAA-Ts) that represent a new and potentially effective nontoxic therapeutic approach for patients with relapsed or refractory solid tumors.
The Phase 1 study led by Children’s National pediatric oncologists Holly Meany, M.D., and Amy B. Hont, M.D., represented the first in-human trial investigating the safety of administering TAA-Ts that target Wilms Tumor gene 1, a preferentially expressed antigen of melanoma and survivin in patients with relapsed/refractory solid tumors.
“These are exciting clinical results using a novel ‘first in-human’ T cell therapy,” said Catherine Bollard, MB.Ch.B., M.D., director of the Center for Cancer and Immunology Research at Children’s Research Institute. “This T cell therapy was safe and appeared to prolong patients’ time to progression which suggests that we can now use this novel treatment as a combination therapy to hopefully achieve long-term remissions in pediatrics and adults with relapsed/refractory solid tumors.”
During the Phase 1 trial, TAA-Ts products were generated from autologous peripheral blood and were infused over three dose levels. Patients were then eligible for up to eight infusions that were administered four to seven weeks apart.
Of the 15 evaluable patients, 11 were with stable disease or better at 45 days post-infusion and were defined as responders. Patients who were treated at the highest dose level showed the best clinical outcomes, with a 6-month progression-free survival rate of 73% after TAA-Ts infusion, an improvement as compared with prior therapy.
Overall, the Phase 1 trial of TAA-Ts resulted in safely induced disease stabilization and was associated with antigen spreading and a reduction in circulating tumor-associated antigen DNA levels in patients with relapsed/refractory solid tumors before infusion.
“The T cell immunotherapy regimen resulted in prolonged disease stabilization in patients who previously experienced rapid tumor progression,” said Dr. Meany. “The therapy could prove to be an important component of immunotherapy for patients with solid tumor malignancies,” she added.
The other researchers that contributed to this work are as follows: Amy B. Hont, M.D.; C. Russell Cruz, M.D., Ph.D.; Robert Ulrey, M.S.; Barbara O’Brien, B.S.; Maja Stanojevic, M.D.; Anushree Datar, M.S.; Shuroug Albihani, M.S.; Devin Saunders, B.A.; Ryo Hanajiri, M.D., Ph.D.; Karuna Panchapakesan, M.S.; Sam Darko, M.S.; Payal Banerjee, M.S.; Maria Fernanda Fortiz, B.S.; Fahmida Hoq, MBBS, M.S.; Haili Lang, M.D.; Yunfei Wang, Dr.PH.; Patrick J. Hanley, Ph.D.; Jeffrey S. Dome, M.D., Ph.D.; Catherine M. Bollard, M.D.; and Holly J. Meany, M.D.


Children’s National Health System researchers Richard Jonas, M.D., Catherine Bollard, M.B.Ch.B., M.D., and Nobuyuki Ishibashi, M.D., have been awarded a $2.5 million, three-year grant from the National Institutes of Health (NIH) to conduct a single-center clinical trial at Children’s National. The study will involve collaboration between the Children’s National Heart Institute, the Center for Cancer and Immunology Research, the Center for Neuroscience Research and the Sheikh Zayed Institute for Pediatric Surgical Innovation.
The goal of the study will be to optimize brain development in babies with congenital heart disease (CHD) who sometimes demonstrate delay in the development of cognitive and motor skills. This can be a result of multiple factors including altered prenatal oxygen delivery, brain blood flow and genetic factors associated with surgery including exposure to the heart lung machine.
The award will be used to complete three specific aims of a Phase 1 safety study as described in the NIH grant:
“NIH supported studies in our laboratory have shown that MSC therapy may be extremely helpful in improving brain development in animal models after cardiac surgery,” says Dr. Ishibashi. “MSC infusion can help reduce inflammation including prolonged microglia activation that can occur during surgery that involves the heart lung machine.”
In addition the researchers’ studies have demonstrated that cell-based intervention can promote white matter regeneration through progenitor cells, restoring the neurogenic potential of the brain’s own stem cells that are highly important in early brain development.
The Phase 1 clinical trial is being implemented in two stages beginning with planning, regulatory documentation, training and product development. During the execution phase, the trial will focus on patient enrollment. Staff from the Cellular Therapy Laboratory, led by director Patrick Hanley, Ph.D., manufactured the BM-MSC at the Center for Cancer and Immunology Research, led by Dr. Bollard. The Advanced Pediatric Brain Imaging Laboratory, led by Catherine Limperopoulos, Ph.D., will perform MR imaging.
The phase 1 safety study will set the stage for a phase 2 effectiveness trial of this highly innovative MSC treatment aimed at reducing brain damage, minimizing neurodevelopmental disabilities and improving the postoperative course in children with CHD. The resulting improvement in developmental outcome and lessened behavioral impairment will be of enormous benefit to individuals with CHD.


Following the noted success of CAR-T cells in treating leukemia, Eugene Hwang, M.D., and a team of physicians at Children’s National are studying the efficacy of using these white blood cell “armies” to fight central nervous system (CNS) tumors.
Following the noted success of CAR-T cells in treating leukemia, physicians at Children’s National are studying the efficacy of using these white blood cell “armies” to fight central nervous system (CNS) tumors. Employing a strategy of “supertraining” the cells to target and attack three tumor targets as opposed to just one, Eugene Hwang, M.D., and the team at Children’s are optimistic about using this immunotherapy technique on a patient population that hasn’t previously seen much promise for treatment or cure. The therapy is built on the backbone of T cell technology championed by Catherine Bollard, M.B.Ch.B., M.D., director of the Center for Cancer and Immunology Research, which is only available at Children’s National. Hwang sees this trial as an exciting start to using T cells to recognize resistant brain cancer. “We have never before been able to pick out markers on brain cancer and use the immune system to help us attack the cancer cells. This strategy promises to help us find treatments that are better at killing cancer and lessening side effects,” he says.
This Phase 1 dose-escalation is designed to determine the safety and feasibility of rapidly generated tumor multiantigen associated specific cytotoxic T lymphocytes (TAA-T) in patients with newly diagnosed diffuse intrinsic pontine gliomas (DIPGs) or recurrent, progressive or refractory non-brainstem CNS malignancies. Pediatric and adult patients who have high-risk CNS tumors with known positivity for one or more Tumor Associated Antigens (TAA) (WT1, PRAME and/or surviving) will be enrolled in one of two groups: Group A includes patients with newly diagnosed DIPGs who will undergo irradiation as part of their upfront therapy and Group B includes patients with recurrent, progressive or refractory CNS tumors including medulloblastoma, non-brainstem high-grade glioma, and ependymoma, among others. TAA-T will be generated from a patient’s peripheral blood mononuclear cells (PBMCs) or by apheresis. This protocol is designed as a phase 1 dose-escalation study. Group A patients: TAA-T will be infused any time >2 weeks after completion of radiotherapy. Group B patients: TAA-T will be infused any time >2 after completing the most recent course of conventional (non-investigational) therapy for their disease AND after appropriate washout periods as detailed in eligibility criteria.
For more information about this trial, contact:
Eugene Hwang, M.D.
202-476-5046
ehwang@childrensnational.org
Click here to view Open Phase 1 and 2 Cancer Clinical Trials at Children’s National.
The Children’s National Center for Cancer and Blood Disorders is committed to providing the best care for pediatric patients. Our experts play an active role in innovative clinical trials to advance pediatric cancer care. We offer access to novel trials and therapies, some of which are only available here at Children’s National. With research interests covering nearly aspect of pediatric cancer care, our work is making great advancements in childhood cancer.
Karun Sharma, M.D., is working with AeRang Kim, M.D., Ph.D., to evaluate the use of ThermoDox®, a heat-activated chemotherapy drug, in combination with noninvasive magnetic resonance-guided high-intensity focused ultrasound (MR-HIFU) to treat refractory or relapsed solid tumors in children and young adults.
A Phase I Study of Lyso-thermosensitive Liposomal Doxorubicin (LTLD, ThermoDox®) and Magnetic Resonance-Guided High Intensity Focused Ultrasound for Relapsed or Refractory Solid Tumors in Children, Adolescents, and Young Adults.
This study is looking to determine the maximum tolerated dose (MTD) and recommended phase 2 dose (RP2D) of lyso-thermosensitive liposomal doxorubicin (LTLD), a heat-activated formulation of liposomal doxorubicin with unique property of heat-activated release of doxorubicin, administered in combination with magnetic resonance-guided high-intensity focused ultrasound (MR-HIFU) in children with relapsed/refractory solid tumors.
MR-HIFU is an innovative device that provides precise and controlled delivery of heat inside a tumor using an external applicator. Unlike other heating systems used in local therapy, MR-HIFU is entirely non-invasive and does not use any radiation. Integration of MR imaging allows for real-time temperature monitoring for accurate and precise targeting of tumors. LTLD is a novel formulation of doxorubicin with the unique property of heat-activated release. This selective drug delivery mechanism allows for local and rapid release of doxorubicin in high concentrations in tumors when heated. This novel combination may potentiate known effective therapy to improve local control and drug delivery without increasing toxicity.
Children’s National Health System and Celsion Corp, a leading oncology drug-development company, were the first to launch a clinical study in the U.S. that evaluates the use of ThermoDox® with MR-HIFU. Learn more about the clinical trial.
For more information about this trial or other trials available at Children’s National, contact:
Melissa Salerno
Clinical Research Program Manager
202-476-2142
msalerno@childrensnational.org
View more open phase 1 and phase 2 cancer clinical trials at Children’s National.
The Children’s National Center for Cancer and Blood Disorders is committed to providing the best care for pediatric patients. Our experts play an active role in innovative clinical trials to advance pediatric cancer care. We offer access to novel trials and therapies, some of which are only available here at Children’s National. With research interests covering nearly aspect of pediatric cancer care, our work is making great advancements in childhood cancer.
“We found that some patients diagnosed with standard tools underwent much more treatment than necessary or intended,” said Eugene Hwang, M.D.
Eugene I. Hwang, M.D., a neuro-oncologist in the Center for Cancer and Blood Disorders, and other researchers at Children’s National Health System, Seattle Children’s Hospital and Research Institute, the Fred Hutchinson Cancer Research Center and the Hopp-Children’s Cancer Center at the NCT Heidelberg recently published the results of a clinical trial focusing on children with histologically diagnosed supratentorial primitive neuroectodermal tumors (CNS-PNET) and pineblastomas (PBLs).
The clinical trial, published online October 17, 2018 in the Journal of Clinical Oncology, included children and adolescents aged 3-22 with these brain cancers who were randomly assigned to receive carboplatin during radiation and/or isotretinoin after the standard intensive therapy (high-dose craniospinal radiation and months of inpatient chemotherapy). Importantly, because each patient was treated prospectively according to the clinical trial design, the conclusions related to tumor biology were felt to be less affected by varied treatment plans.
“This trial really highlighted the importance of new molecular testing methods in accurately diagnosing some of the brain cancers included in the trial. We found that some patients diagnosed with standard tools underwent much more treatment than necessary or intended.” says Dr. Hwang. “Kids who aren’t receiving the right form of cancer treatment may not get better despite months and months of intensive treatment.”
During this clinical trial, 85 participants with institutionally-diagnosed CNS-PNETs/PBLs were enrolled. Out of the 60 patients with sufficient tissue, 31 were non-pineal in location, 22 of which represented tumors that did not fit in the diagnoses intended for trial inclusion.
The researchers discovered that patient outcomes across each molecularly-diagnosed tumor type were strikingly different. Patients with molecularly-confirmed supratentorial embryonal tumors/PBLs exhibited a five-year event free survival (EFS) and an overall survival rate of 62 percent and 78.5 percent, respectively. However, patients with molecularly-classified high-grade gliomas (HGGs) had a five-year EFS of 5.6 percent and OS of 12 percent, showing no benefit even with the chemotherapy and craniospinal radiation.
Researchers determined that for patients with CNS-PNETs/PBLs, prognosis is considerably better than previously assumed when molecularly-confirmed HGG are removed. Dr. Hwang and co-authors concluded that molecular diagnosis can greatly aid standard pathological diagnostic tools, preventing unnecessary intensive therapy for some patients while enabling more rational treatment for others.
“The findings from our clinical trial have highlighted the immense challenges of histology-based diagnosis for some types of pediatric brain tumors, and the enormous importance this has for children with brain cancer,” Dr. Hwang says. “We hope that ultimately our study will pave the way for molecular profiling to become a standard component of initial diagnosis.”