Protecting the fetal brain from harm
Ongoing placental dysfunction and allopregnanolone loss, not the increase that was expected due to stress, may alter cortical development in complicated pregnancies and put babies at risk, says Anna Penn, M.D., Ph.D.
Researchers long have known that allopregnanolone (ALLO), a derivative of the hormone progesterone, is produced in adults’ brains during times of acute stress and modulates how easily the brain’s neurons fire. ALLO also is produced in the placenta during fetal development, one of more than 200 different hormones that each uniquely contribute to fostering a smooth pregnancy and maintaining a fetus’ overall health. Although ALLO is thought to protect the developing brain in pregnancies complicated by conditions that might harm it, such as high blood pressure, how its levels evolve during pregnancy and in newborns shortly after birth has remained unknown.
Now, a new study presented during the Pediatric Academic Societies (PAS) 2018 annual meeting suggests that the placenta ramps up ALLO production over the second trimester, peaking just as fetuses approach full term.
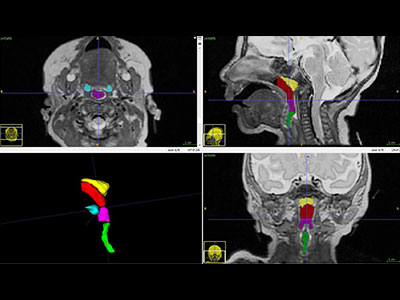
To investigate this phenomenon, Anna Penn, M.D., Ph.D., a neonatologist/neuroscientist at Children’s National Health System, and colleagues created a designer experimental model to study how premature loss of ALLO alters orderly brain development. Knowing more about the interplay between ALLO and normal development of the cortex, the outer layer of the cerebrum, is a first step that could lead to strategies to rescue this vital brain region.
“The cortex is basically the brain’s command-and-control center for higher functions. In our experimental model, it develops from the middle of gestation through to the end of gestation. If ALLO levels are disrupted just as these cells are being born, neurons migrating to the cortex are altered and the developing neural network is compromised,” says Dr. Penn, senior author of the research presented at PAS 2018. “We’re concerned this same phenomenon occurs in human infants whose preterm birth disrupts their supply of this essential hormone.”
To better understand the human placental hormone pattern, the research team analyzed cord blood or serum samples collected within the first 36 hours of life for 61 preterm newborns born between 24 to 36 gestational weeks. They compared those preemie samples with samples drawn from 61 newborns carried to term who were matched by race, gender, size for gestational age, delivery method and maternal demographics.
They used liquid-chromatography-tandem mass spectrometry, a technique that can precisely analyze trace levels of compounds, to compare levels of 27 different steroids, including ALLO and its precursors as well as better-known adrenal gland hormones, such as cortisol and 17-Hydroxyprogesterone.
“Pregnancies complicated by hypertension tended to correlate with lower ALLO levels, though this finding did not reach statistical significance. This suggests that ongoing placental dysfunction and ALLO loss, not the increase that we expected to be caused by stress, may alter cortical development in these pregnancies and put babies at risk,” Dr. Penn adds. “In addition, having the largest neonatal sample set to date in which multiple steroid hormones have been measured can provide insight into the shifting hormone patterns that occur around 36 weeks gestation, just prior to term. Hopefully, restoring the normal hormonal milieu for preemies or other at-risk newborns will improve neurological outcomes in the future.”
In addition to Dr. Penn, study co-authors include Caitlin Drumm, MedStar Georgetown University Hospital; Sameer Desale, MedStar Health Research Institute; and Kathi Huddleston, Benjamin Solomon and John Niederhuber, Inova Translational Medicine Institute.